")
Assessing and managing eye injuries
Related content
Introduction
Injuries to the eye are common. Many are minor but, if not treated quickly and appropriately, can lead to sight-threatening complications. Other injuries are severe, and even with expert management sight can be lost. Prevention of blindness from eye injuries requires:

- injury prevention (health promotion including advocacy)
- early presentation by the patient (health promotion and health worker training)
- accurate assessment (good primary eye care and first aid)
- prompt referral of serious injuries requiring specialist management.
Taking a history
The history obtained following trauma should be as precise as possible. The history should include details of:
- anything that hit the eye
- what the patient was doing when the eye was injured
- any treatment given.
Particular attention is required if a foreign body is involved or if the injury may have perforated the globe. For example, a history of a blow to the eye by a broomstick suggests blunt trauma, but if the weapon was the tip of a rotten broomstick, one would look for a retained foreign body; if the fist was the weapon but the assailant was wearing a ring, one would look for lacerations to the globe as well as contusion or bruising of the lids and orbit. Human bites, or penetrating injuries caused by dirty or used kitchen utensils, may cause fulminant infection, so the patient should be treated with systemic antibiotics. When metal hits metal (such as hammer and chisel), the velocity of the metal fragment is enough to leave the slightest of marks on the cornea as it tracks through the globe to the vitreous cavity, whereas the grit from a coal engine embeds itself in the corneal epithelium as a corneal foreign body. Intraocular foreign bodies, such as glass, may be inert but the reaction caused by a copper fragment can destroy the retina within days. With chemical injuries it is important to know the type of substance that caused the burn, and how long the substance had contact with the eye. An irritant such as pepper would cause discomfort but no actual damage, alkali and hydrofluoric acid burns are the most dangerous, while acid burns caused by chemicals with a low pH tend to be less severe than alkali burns.
Managing eye injuries: outline of management principles
Prophylaxis for tetanus infection is required for a patient with lacerations, particularly if dirty.
Corneal abrasions
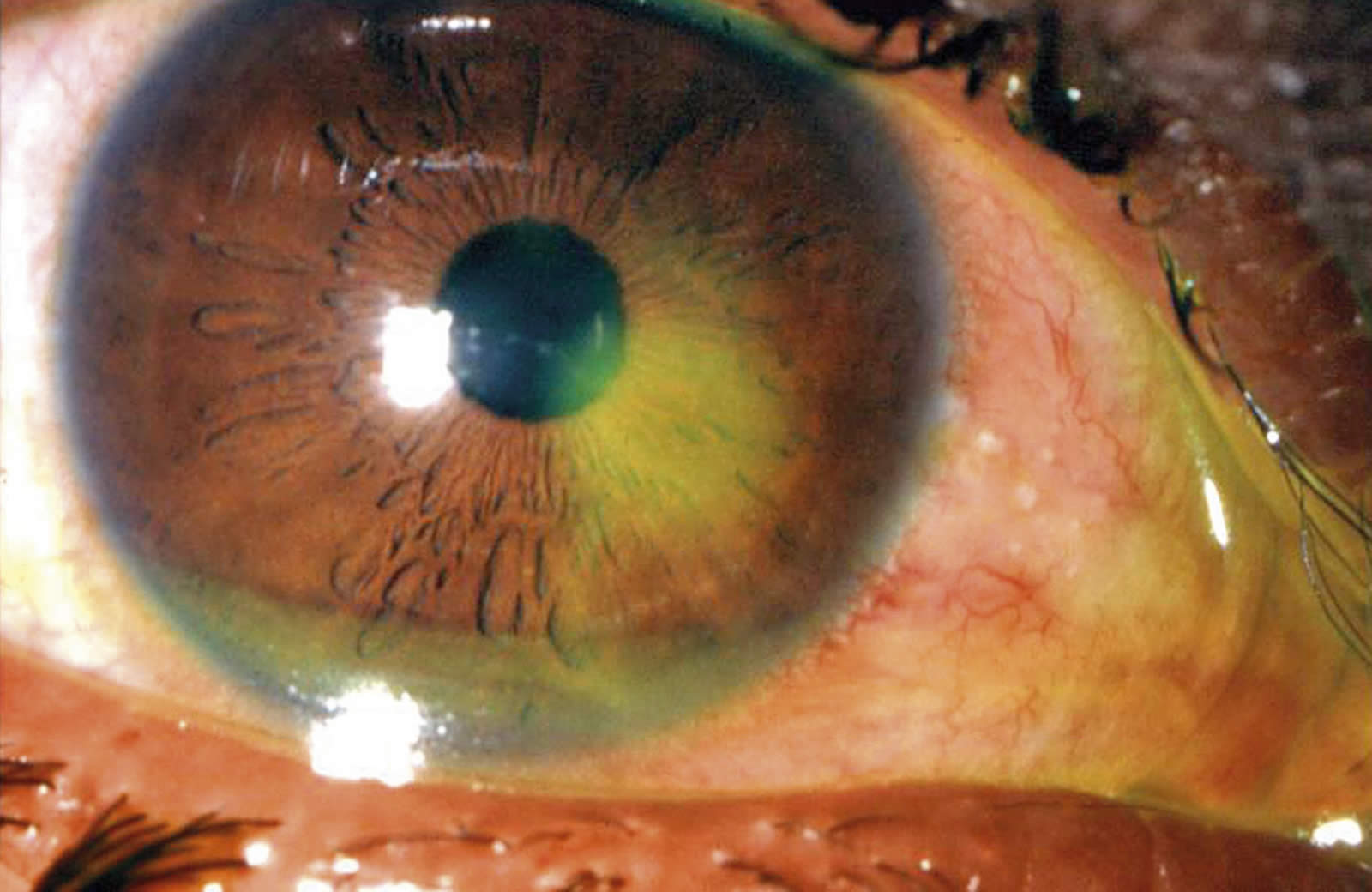
Corneal foreign bodies can be removed after adequate topical anaesthesia under magnification with good illumination. A corneal abrasion is often caused by a finger, resulting in an extremely painful eye that can be examined once topical anaesthetic has been instilled. Fluoroscein staining will indicate an epithelial defect (Figure 1). Management is with an antibiotic and eye padding for one day.
Damage to the cornea may occur when welding without protective goggles. Diffuse punctate staining is visible over the whole cornea when stained with fluoroscein, and the symptoms are similar to that of a corneal abrasion, but usually in both eyes. Management is as for abrasion.
Penetrating injury (open injury of the globe)
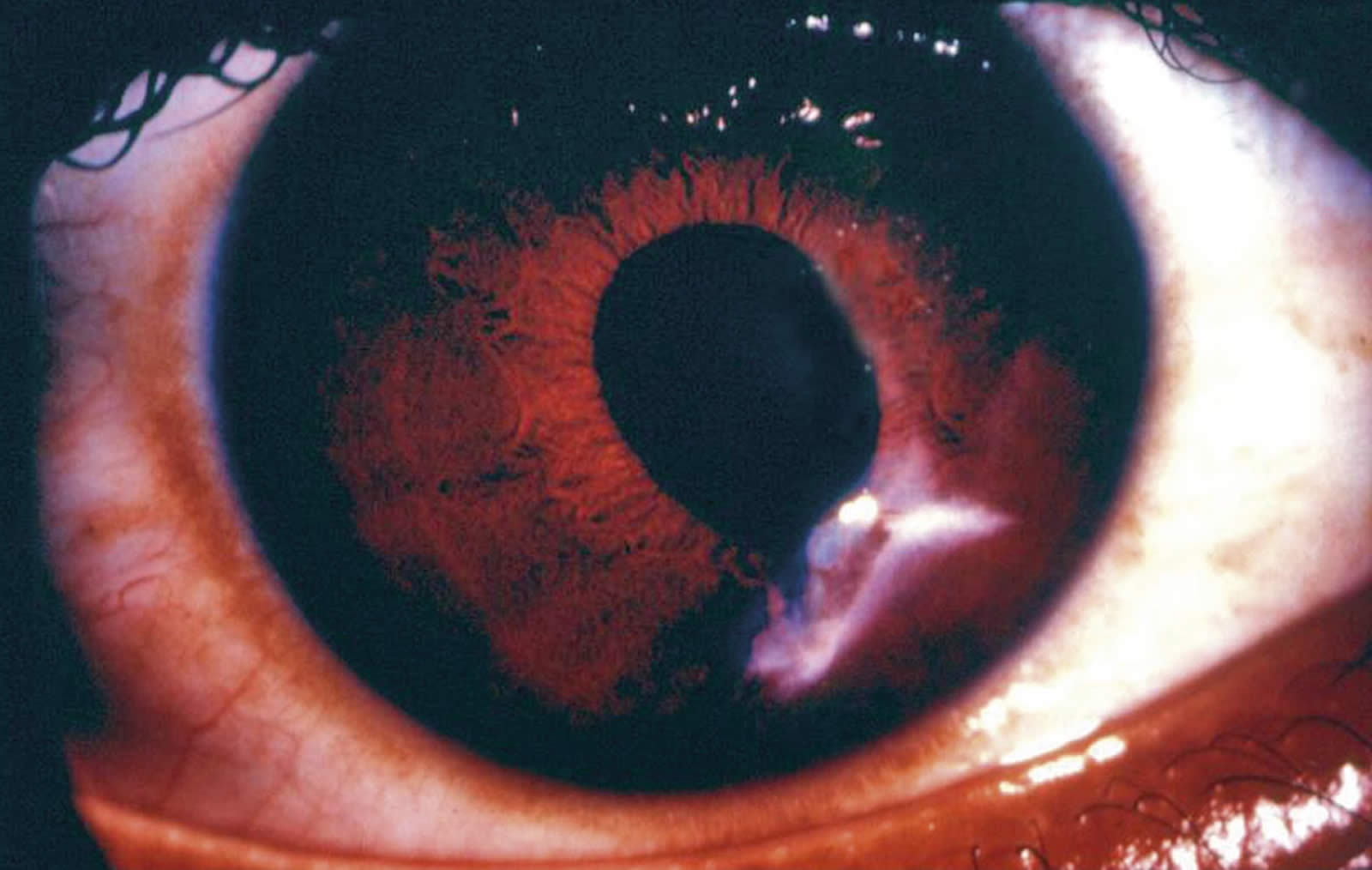
Any open injury of the globe needs emergency referral to an eye specialist. A shield only should be placed over the injured eye – eye pads must not be used so as to avoid any pressure on the eye. A globe ruptured by blunt trauma (e.g. a blow by a fist) should be treated in the same way as a penetrating injury, even if the rupture injury is sub-conjunctival (Figure 2).
Lid and canalicular lacerations
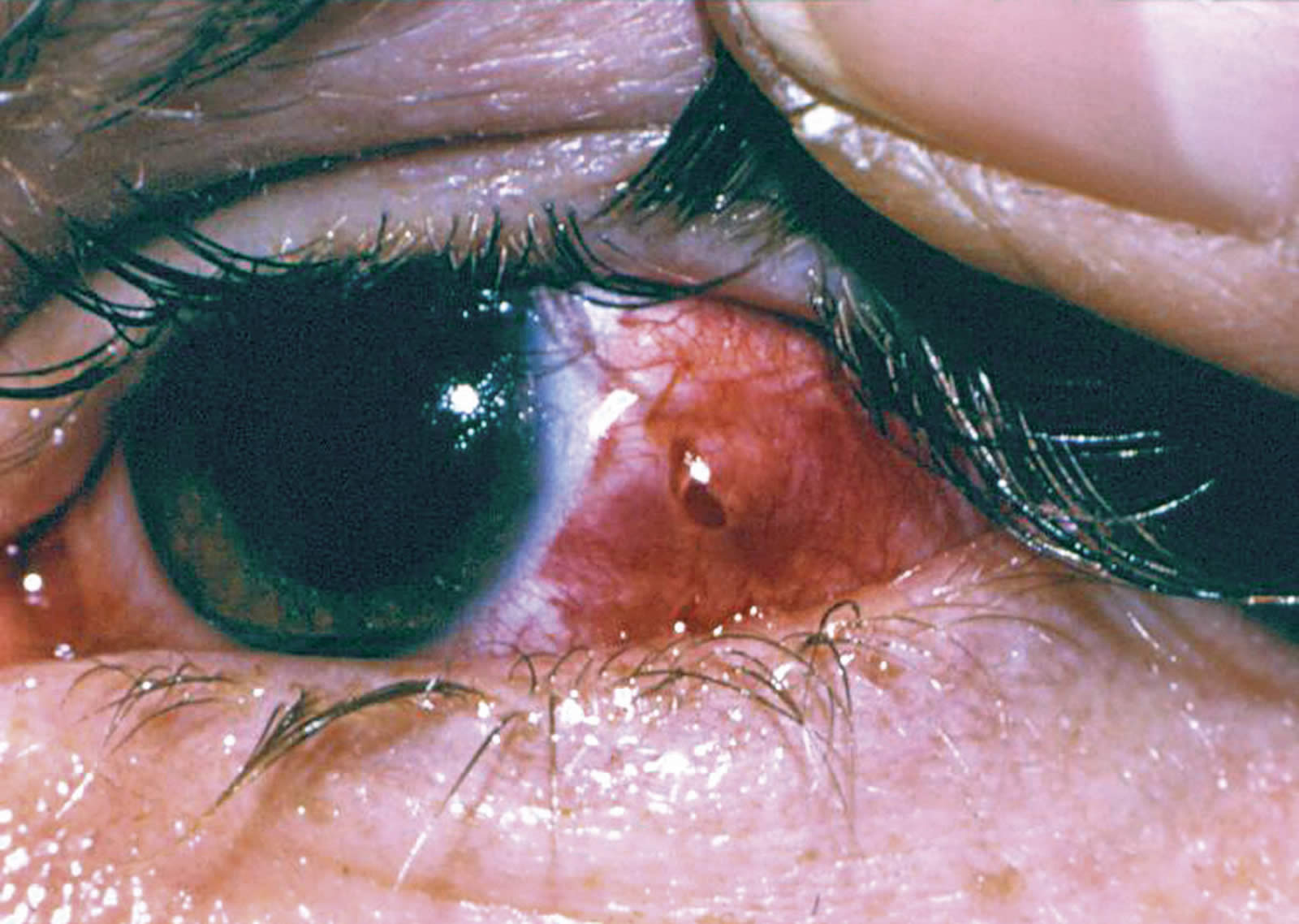
Simple lacerations can be sutured. Septic lacerations should be cleaned and treated with systemic antibiotics. Delayed primary closure may be advisable. Lacerations involving the lid margins should also be referred to a specialist who is familiar with the technique of opposing the lid margins with fine precision. Medial canthus injuries should be assessed to see if there is a tear of the lower canaliculus (a lacrimal probe can be used). If damaged, the patient should be referred to an eye specialist for canalicular repair (Figure 3).

Haemorrhage
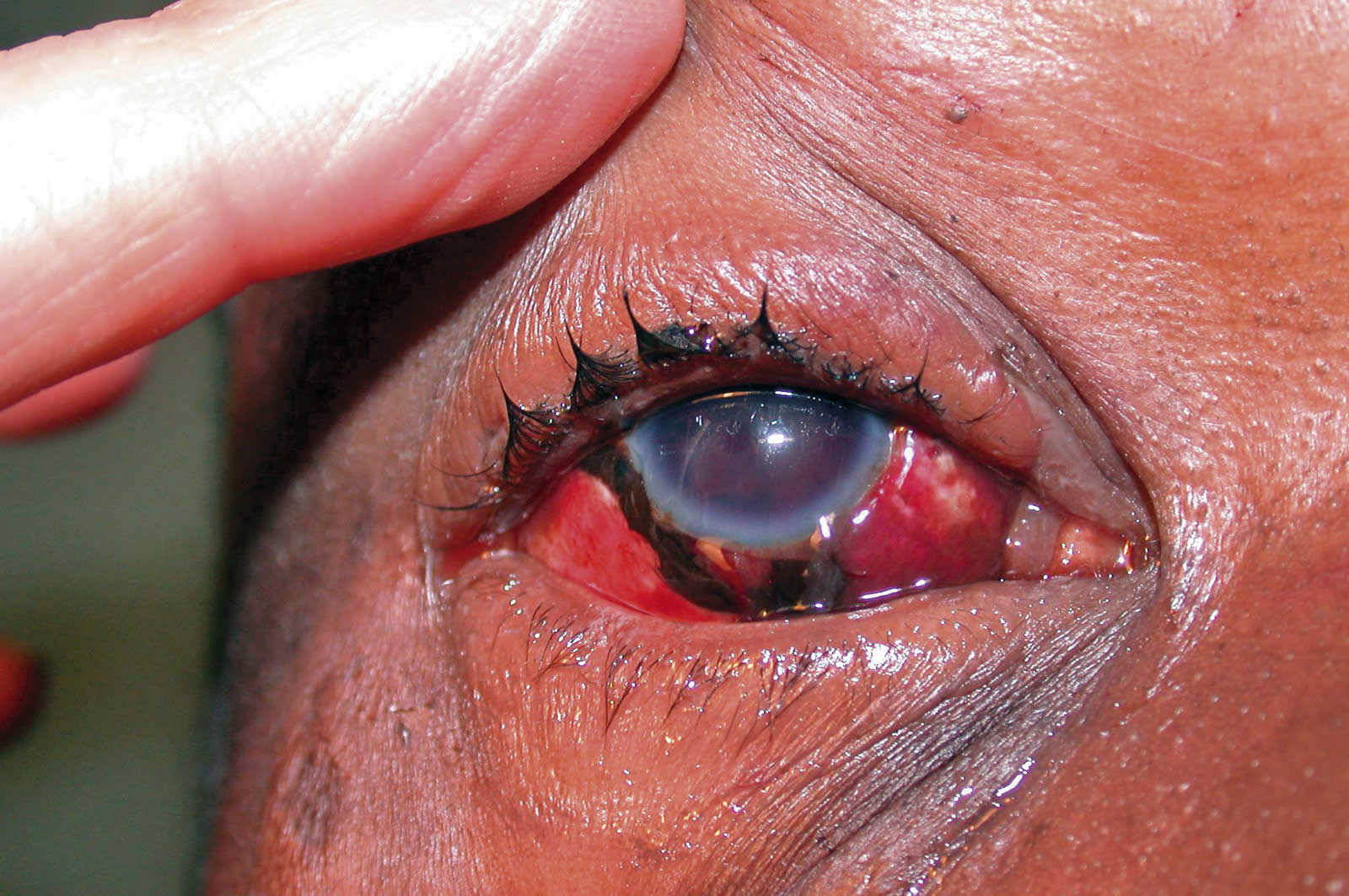
A sub-conjunctival haemorrhage is quite common after trauma and can be managed conservatively (Figure 4).
However, occasionally it can be the only sign of a ruptured globe, when it may be associated with a low intraocular pressure (IOP) and an abnormally deep anterior chamber. Blood in the anterior chamber is called hyphaema. It usually follows a blunt injury and results from tearing of the iris. The pupil may be dilated. Most hyphaema clear within five to six days with conservative treatment. The sight- threatening complications of hyphaema are caused by raised IOP, which is managed by oral acetazolamide (Diamox). Surgical washout of a hyphaema is very rarely required and carries particular risks, so should only be resorted to for specific indications. These include:
- corneal staining from persistent hyphaema
- increased IOP of more than 45 mm Hg for more than four days
- sickle cell disease with failure of the hyphaema to resolve and raised IOP.
The risk of further bleeding into the eye is increased by the use of aspirin, and may be decreased by topical steroids. Patients should be advised to avoid non-steroidal anti-inflammatory drugs for one week aftera hyphema. Vitreous haemorrhage is a sign of serious intraocular trauma, and is characterised by the loss of the red reflex compared with the other eye. All cases of vitreous haemorrhage should be referred for further examination to exclude globe rupture or perforation, or other sight-threatening complications such as retinal detachment (Figures 5 & 6).

Lens damage
The lens may be subluxated or even dislocated. The intraocular pressure may increase in the acute phase and a lens extraction may be indicated. Both blunt and perforating injury may cause a cataract requiring extraction, either very soon after injury if it is causing complications, or later when the eye is quiet and recovered from the injury.
Orbital injuries
Proptosis or diplopia (double vision) suggests serious eye injury for which specialist assessment and management is required.
Burns to the eye
Burns to the eye may affect the eyelids, conjunctiva or cornea. It is important to keep the cornea moist and free from exposure. The first aid management is to apply antibiotic ointment generously all over the conjunctiva, cornea and burned eyelids. An eye pad should not be placed over the eye as this may ulcerate the cornea. The patient may require skin grafting of the eyelids.
Chemicals in the eye
The first aid management of chemicals in the eye is immediate and profuse irrigation with clean water after instilling local anaesthetic drops. The patient should lie flat while water is poured into the eye generously for at least 15 minutes (see page 109). After this time the eye can be examined with fluorescein to see if there is any evidence of corneal ulceration. If there is ulceration, the patient should be given topical antibiotics, and an eye pad and seen daily. Many chemical injuries are caused by acid (e.g. exploding car battery), and these usually have a good prognosis as the acid damages only the superficial layers of the cornea. Alkali burns (e.g. ammonia) are less common, but much more severe. They should be referred to an ophthalmologist, as they will require intensive topical steroids, tetracycline and vitamin C drops.
Eye removal – evisceration or enucleation?
If the eye is blind to light and painful, then removal should be considered. Evisceration is thought to carry a risk of sympathetic ophthalmia, but there is little evidence to support this. Evisceration may be more appropriate (for non-malignant conditions) in developing countries, because the procedure is simpler than enucleation, the results offer better cosmetic results and there is less danger of systemic infection if the eye is infected. It can also be performed under local anaesthesia. Table 1. Definitions of terms used to describe eye injuries
| Term | Definition |
|---|---|
| Abrasion | Defect of the corneal epithelium. Stains with fluorescein. Usually heals within 24 – 48 hours |
| Contusion | Result of blunt injury, either at site of impact or distant to it |
| Closed injury | The wall of the globe is intact but structures inside the eye are damaged |
| Rupture | Jagged open injury due to blunt injury, often away from the site of injury at the weakest points of the globe: concentric to the limbus, just behind the insertion of the extraocular muscles or at the equator |
| Open injury | A full thickness break in the wall of the eye; can follow either sharp or severe blunt injury |
| Lamellar laceration | Partial thickness wound caused by a sharp object |
| Laceration | Full thickness penetration |
| Penetration | Entry wound only |
| Perforation | ‘Through and through’ injury; an injury that goes right through the eye, causing both entry and exit wounds |

In summary
Managing ophthalmic trauma is challenging. Clinical and surgical skills and equipment vary from place to place and country to country so that the management of serious eye injury requires a variety of alternative strategies. In principle, if a health care worker can diagnose and treat a condition and recognise the complications, then he or she can manage that case.
Corneal abrasions, conjunctival, tarsal, superficial corneal foreign bodies and small lid lacerations not involving the lid margins, can be managed by ophthalmic nurses and general practitioners. Injuries such as deep corneal foreign bodies and large hyphaemas should be managed in centres where slit lamp examinations can be performed and intraocular pressure (IOP) can be measured. Open globe injuries, lid lacerations involving the lid margin or canaliculi, blow out fractures with diplopia in the primary position and any potential intraocular foreign body should be referred to a well equipped eye care centre.
The commonest pitfalls in dealing with ocular trauma are:
- missed tarsal foreign bodies (Figure 7)
- missed intraocular foreign bodies
- confusing corneal ulcers with abrasions
- missed scleral lacerations and ruptures
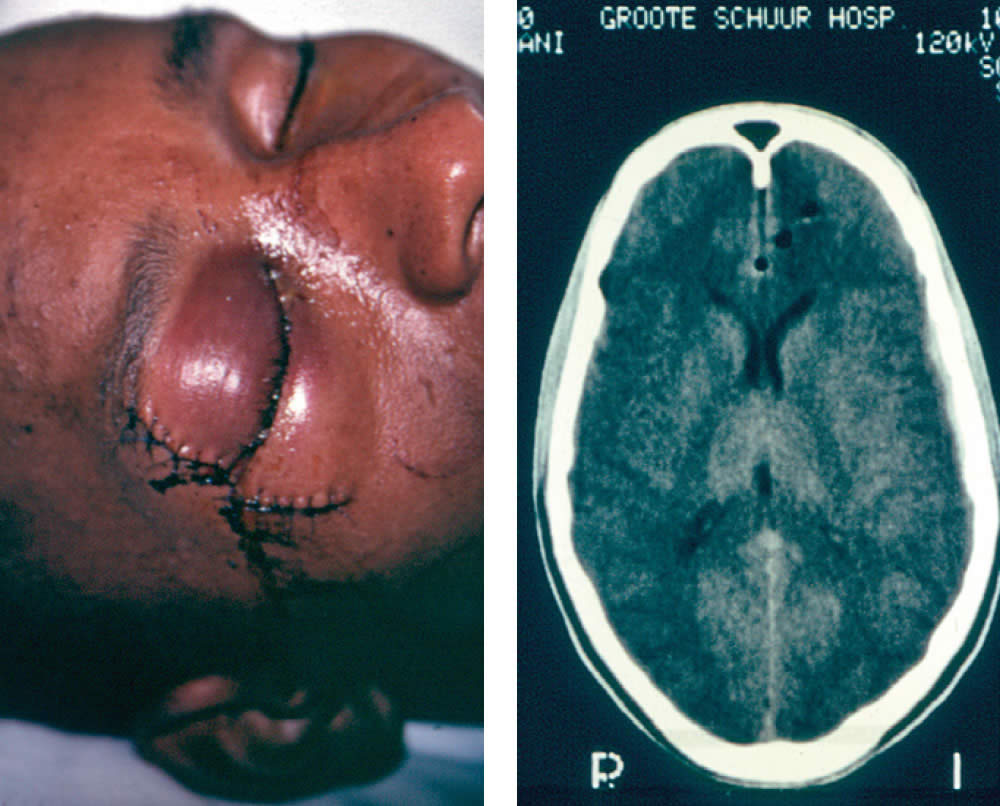
- missed cranial injuries in sharp orbital trauma (Figures 8 & 9).
This editorial lays out guidelines on the assessment and management of trauma to the eye. Practitioners may manage patients differently according to the availability of equipment, skills, finances and transport.
Table 2. Ocular signs and their implications following ocular trauma
| Structure | Appearance and associated features | Implication |
|---|---|---|
| Lids | Lacerations of lid margins | Will require accurate repair |
| Puncture wounds | Check for globe perforation | |
| Involvement of medial canthus | Check for canalicular damage | |
| Conjunctiva | Sub-conjunctival haemorrhage | Usually harmless, but exclude perforation if the IOP is low |
| Sclera | Grey or brown discolouration on sclera | Check for scleral perforation or laceration |
| Cornea | Foreign body | Remove foreign body |
| Abrasion | Treat with antibiotic and pad | |
| Multiple staining areas following arc welding | Treat as for an abrasion | |
| Laceration with iris prolapse | Will require urgent repair | |
| Anterior chamber | Blood in the anterior chamber – hyphaema | Usually resolves with conservative treatment; if secondary glaucoma, lower IOP with diamox |
| Pupil | Peaked | Check for laceration with iris prolapse, and refer for abcission repair |
| D shaped – Iris dialysis | Manage conservatively but watch for secondary glaucoma | |
| Lens | Iris tremor – probable lens dislocation | Usually requires removal |
| White lens | Lens damaged resulting in a cataract | |
| Red reflex | No or poor red reflex | Possible vitreous haemorrhage |
| Proptosis | Swollen lids and protruding eye | Medial wall blow out fracture with air in the orbit, orbital contusion or sub-periosteal haematoma |
| Endophthalmos | Eye looks smaller – sunken-in globe | Inferior wall blow-out fracture |