")
Childhood cataract: home to hospital
Related content
Introduction
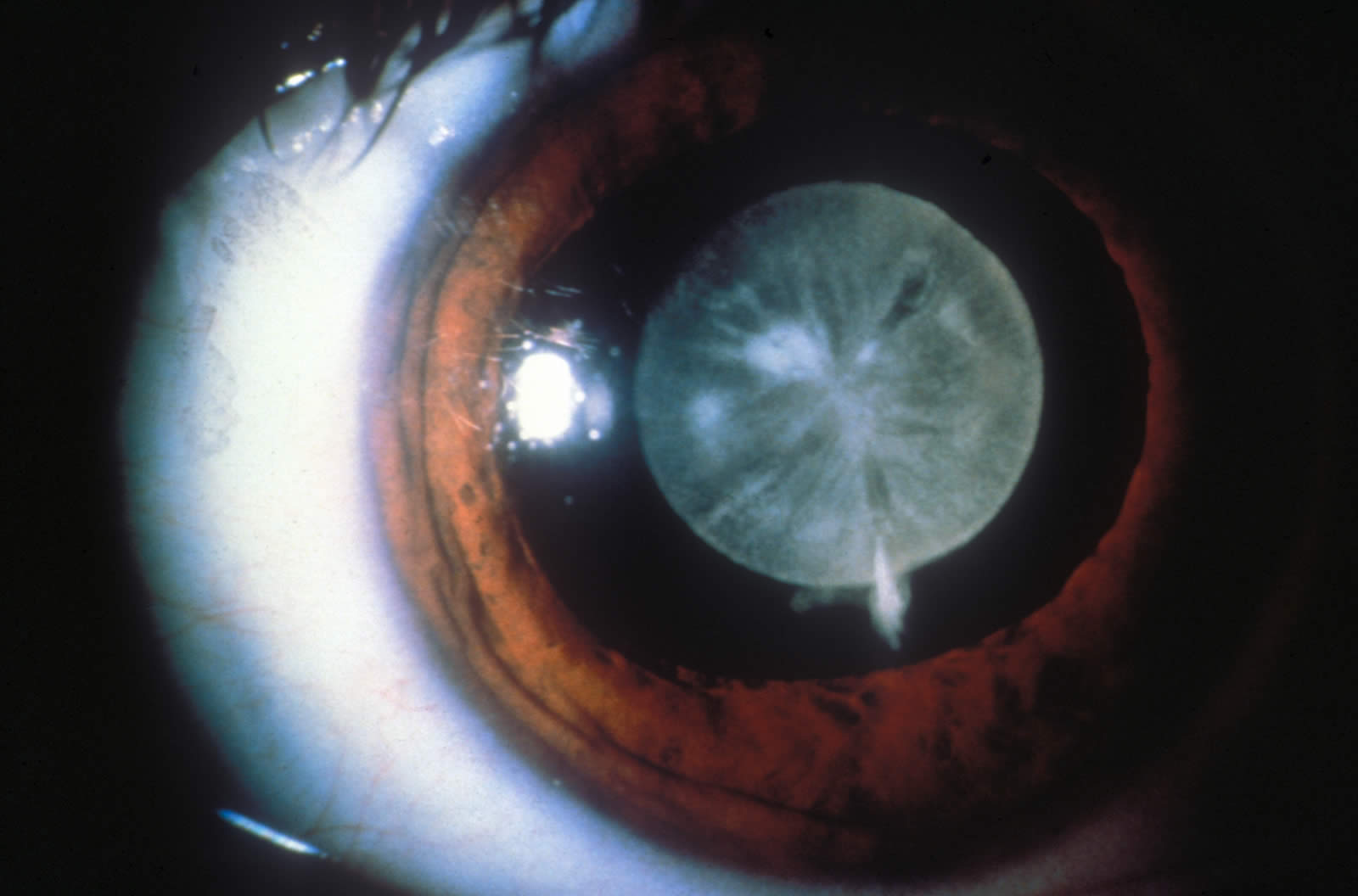
Globally, there are 190,000 children who are blind from cataract.1 Cataract in children may be present at birth (congenital cataract) or may appear anytime during the first few years of life (developmental cataract). Childhood cataract is the most common treatable cause of childhood blindness, being responsible for 10-30% of all childhood blindness. A recent national study in Bangladesh showed that 1 in every 3 blind children is unnecessarily blind from congenital/developmental cataract.2


Restoring sight: four stages of cataract care for children
Restoring sight in a child who is blind from cataract depends on four stages:
- Early detection of blind children within households and communities.
- Eye examination of blind children and referral of children with cataract.
- Good quality cataract surgery and optical correction.
- Follow-up care: regular and long-term.
The child’s progress through these stages depends on a series of journeys: travel from home to hospital for cataract surgery; from hospital to home after discharge; then again from home to hospital for follow-up on more than one, and often many occasions. Although significant progress has been made in surgical management of cataract, uptake of cataract surgery in children is low in most resource-poor countries.3 This article discusses barriers to cataract services specific to children and proposes a framework for developing comprehensive cataract care. Suggestions are based on our experiences in Bangladesh. The framework could be adapted for other countries as we strive to achieve the aim of VISION 2020 to eliminate avoidable blindness in children.
Barriers
Barriers to early detection of blind children with cataract
In resource-poor countries, particularly in rural areas, a child with cataract often stays at home as parents are unaware that the child is suffering from a treatable condition. Barriers to early detection are related to the difficulty in recognising childhood cataract; beliefs which prevent family members from taking action if they notice a problem, and a lack of knowledge amongst primary level health care providers (traditional and modern) to detect childhood cataract (Box 1).
Barriers and factors influencing eye care provision for children
Barriers to eye examination and referral services
When parents or relatives do recognise that a child is blind, a number of factors might prevent them from taking action: no access to eye care services; family decision not to seek advice; lack of referral or inappropriate advice from traditional or modern health practitioners (Box 2).
Barriers to uptake of cataract surgery in children
Accepting blindness in a child, and acting on the advice that the child needs surgery in both eyes, is not easy for parents. Without appropriate counselling, many parents do not accept referral for cataract surgery even when surgery is offered completely free of charge (Box 3).
Barriers to regular and long-term follow up after cataract surgery in children
Unlike cataract surgery in adults, long-term, regular follow-up over several years, and optical correction after surgery, are critical to achieving a good visual outcome. Commitment from parents is required but difficult to achieve. Again, there are major barriers. These include lack of clear communication between hospital staff and parents, lack of motivation of the parents, and financial barriers (Box 4).
Overcoming barriers: developing a framework for care
The barriers at the four critical stages of care for children with cataract are multifaceted, interlinked and span a wide range of factors. Any intervention should address the barriers simultaneously in a co-ordinated way. The following framework proposes a starting point for developing a comprehensive approach to cataract care for children.
Empower communities to recognise childhood cataract and take action
The first step is to raise awareness that cataract can affect children and it can be treated. A mass communication approach (radio, TV, village theatre, public announcements at communal gatherings, etc.) might be appropriate, with special attention to tailoring the message to the perceptions and attitudes of the target communities. Detecting childhood cataract requires a trained eye. Community members can be trained in ‘how to identify a blind child’. Their efforts could be coordinated by a ‘community facilitator’ in each district whose role would be to contact, encourage, facilitate and engage communities to identify childhood blindness and childhood cataract. He or she would also provide support and linkages with hospital and other services (education, rehabilitation). Increased awareness, however, may not be enough as age-old beliefs and attitudes persist. Opportunities for face-to-face discussion should be built into the strategy. Key informants (school teachers, imams, NGO workers) may act as ‘change agents’, changing community attitudes and beliefs about childhood blindness. Finally, however much parents are convinced about the need to seek treatment for a cataract blind child, practical and financial barriers may prevent them from carrying out their intentions. Mechanisms need to be developed locally to provide financial and practical support to families of children with cataract. Local philanthropists, corporate sponsors, government departments and other interested parties should be encouraged to support these children and their families.

Make facilities available for eye examination and referral
Another approach is to train all those likely to be consulted by the parents of a blind child: traditional healers (including ‘untrained village doctors’ and spiritual healers), health workers, medical doctors and general practitioners. Training curricula for all primary eye care workers should specifically cover eye diseases in childhood, including cataract. Outdated messages such as ‘wait for the cataract to mature’ should be corrected (see 10 Key Messages on Childhood Cataract). Ideally, all blind children should receive a free eye examination by an ophthalmologist in their home sub-district. One idea to achieve this is a mobile community child sight clinic led by an ophthalmologist.

Provide good quality eye surgery: paediatric ophthalmology units
High quality surgery for children should be provided by a well-trained team in a well-equipped hospital with linkages to the community-level service providers.
Ensure follow-up care: community clinic and eye hospital
Long term follow-up and postoperative optical correction are essential components of cataract surgical services for children. Children should receive follow-up services from an ophthalmologist either in the eye hospital or in the community clinic. Programmes should adopt a proactive approach, for example by follow-up visits by the ophthalmologist and his team at sub-district level. Communication between hospital and parents needs to be enhanced. Parents need clear instructions for follow-up and opportunities to ask questions. Without engaging parents in the process it is impossible to achieve their commitment for long-term follow-up.

Create long-term partnerships: linking services and encouraging self-help
Sector wide linkages should be developed between eye hospitals, NGOs, primary health care workers, community-based rehabilitation (CBR) workers, educators and other development workers as well as key members of each community.
Counselling at each stage should provide an opportunity to overcome barriers, develop an understanding of the disease, and provide support to the parents.
Self-help groups of families with blind children can empower families, encourage long-term engagement of communities with eye care programmes, provide support to those in need, and create a sustainable framework for community-based eye care. Effort and care are needed to establish such groups and should be supported by the eye care providers in each district.
Conclusion
The framework in this article outlines some basic considerations for establishing community action for children with cataract while at the same time ensuring that the infrastructure is in place to meet the need for services. It proposes that the starting point should always be an understanding of the barriers, as this will help to make the approach appropriate to each setting.
References
1 Gilbert CE, Foster A. Childhood blindness in the context of VISION 2020:The Right to Sight. Bull World Health Organ 2001; 79: 227-232.
2 Muhit M, Gilbert C, Foster A. Causes of Childhood Blindness in Bangladesh: Results of a National Study of 1,935 Children with Blindness and Severe Visual Impairment. (In preparation).
3 Muhit M, Gilbert C. A review of epidemiology and control of childhood blindness. Trop Doct 2003; 33(4):197-201.
Box 1: Barriers to early detection of children with cataract at household and community level
Barriers specific to children with cataract
- Children do not usually complain of symptoms
- Children do not present themselves to health workers
- Visual loss in a very young child is difficult to recognise
- Early cataract is difficult for an untrained observer to recognise
Perceptions and behaviour of family and community members
People may think:
- Cataract occurs only in elderly people
- Congenital blindness cannot be treated
- Familial blindness is ‘a punishment from God’
- Health Education messages are sometimes confusing
- Corneal scar and cataract are thought to be the same condition causing confusion about what can be done
People might:
- Wait for the child to ‘learn to see’
- Wait for the ‘small white spot’ to disappear
- Deny the blindness
- Accept the blindness and decide not to seek advice
Skills, attitude and practice of service providers (traditional and modern)
- Traditional practitioners are often the first people to be consulted because they are trusted, affordable and accessible. However, they lack skills and training to identify children with cataract
Box 2: Barriers to eye examination and referral
Barriers specific to children with cataract
- Cataract may not be a priority among parents of children with multiple disabilities
Perceptions and behaviour of family and community members
- The perception that blindness is caused by vitamin A deficiency prevents parents from travelling to an eye doctor because ‘we know that it is not going to bring any benefit to the child’
- Financial and practical constraints:
- Cost of travel and accommodation for four people (child, mother, male family member, and a neighbour who knows the city)
- Cost of consultation and treatment
- Staying away from work means lost earnings
- The distance to the hospital
- Time to make arrangements and visit the hospital
- Perceived benefits of being blind, such as children can earn money by begging, social service support for blind children, and state benefit for families with a blind child
Skills, attitude and practice of service providers (traditional and modern)
- Primary eye care training often focuses on cataract in adults without teaching about cataract in children
- Traditional healers may not recognise cataract in children, or understand the need, urgency, and how to refer
- General practitioners may not be aware of available paediatric cataract surgical facilities
- Parents may be incorrectly advised to wait for surgery until the child is older, commonly over 12 years of age
- A common presentation time is 6-8 years old, by which stage the parents may be told that it is already too late for treatment
- Contradictory advice from different providers (too early or too late for surgery) cause confusion and may influence parents not to advance further with the treatment
- Doctors do not explain clearly to the parents the risk of amblyopia if surgery is delayed
Lack of services and linkages
- In many areas, there are no trained staff
- Remote rural areas lack referral linkages with the eye hospital
Box 3: Barriers to uptake of cataract surgery in children at tertiary eye centres
- Challenges faced by family members
- Many parents are not aware that surgery is the only treatment for childhood cataract
- Parents often prefer medical treatment or non-invasive treatments (including traditional remedies) to surgical treatment
- Experience of poor outcome of cataract surgery in other children from the same locality or family acts as a strong disincentive to the uptake of surgery
Fear of:
- surgery in young children
- losing life during surgery
- cutting such a ‘small’ eye
- ‘removing eyes’
- ‘removing lens (cataract)’ from child’s eye
- ‘putting lens inside child’s eye’
- travelling to the big city to visit the eye hospital
Financial barriers
- cost of travelling and accommodation for 3/4 members of the family
- fees for consultation, investigations, surgery, post-operative medication, spectacles
- ‘benefit’ of being blind
Box 4: Barriers to follow-up of children after cataract surgery
Barriers specific to children
- Children usually do not complain of worsening vision (for example due to post capsular opacification); they need someone to detect the problem during follow-up
- Children do not present themselves to health workers, they need parents or another adult to decide and act on their behalf
Perceptions and behaviour of family and community members
- Often adult patients are told that there is no need to come back after cataract surgery if they continue to see well. This message is generalised to children leading to the belief that there is no need for long term follow-up in children
- Perception of ‘good surgery’: ‘When the surgery is good, you don’t need to go back to the doctor’
- Perception of ‘bad surgery’:
- ‘They told us to go back to hospital, but if the surgery is not good and the child can’t see well, what’s the point of going back?’
- Perceived cost of follow-up visit and treatment (on the basis of the cost of initial visit and surgery)
Skills, attitudes and practice of service providers
- Service providers may not be aware of the need for follow-up examinations by an eye doctor
- Lack of clear communication: ‘No one told us to go back for follow-up’, ‘Went for follow-up after two weeks and the doctor said everything is fine’
Lack of services and linkages
- Lack of referral linkages between local service providers and eye hospitals
- Lack of counselling services for the parents to motivate them to attend for follow-up visits for the child