")
Vernal keratoconjunctivitis
Related content
Why is allergic eye disease a problem for eye workers?
Why is allergic eye disease, and vernal keratoconjunctivitis (VKC) in particular, a problem for eye workers and patients in hot climates?
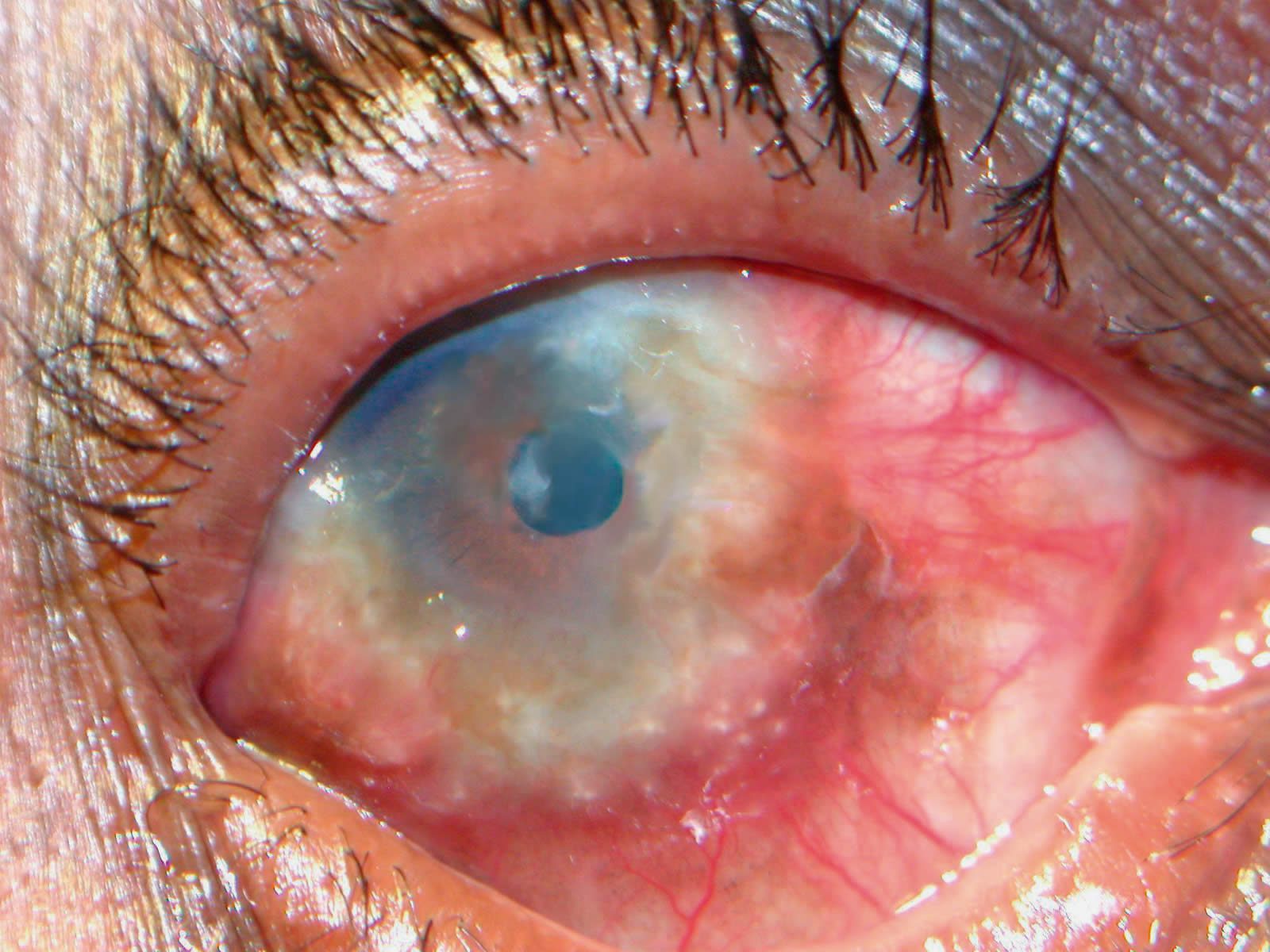
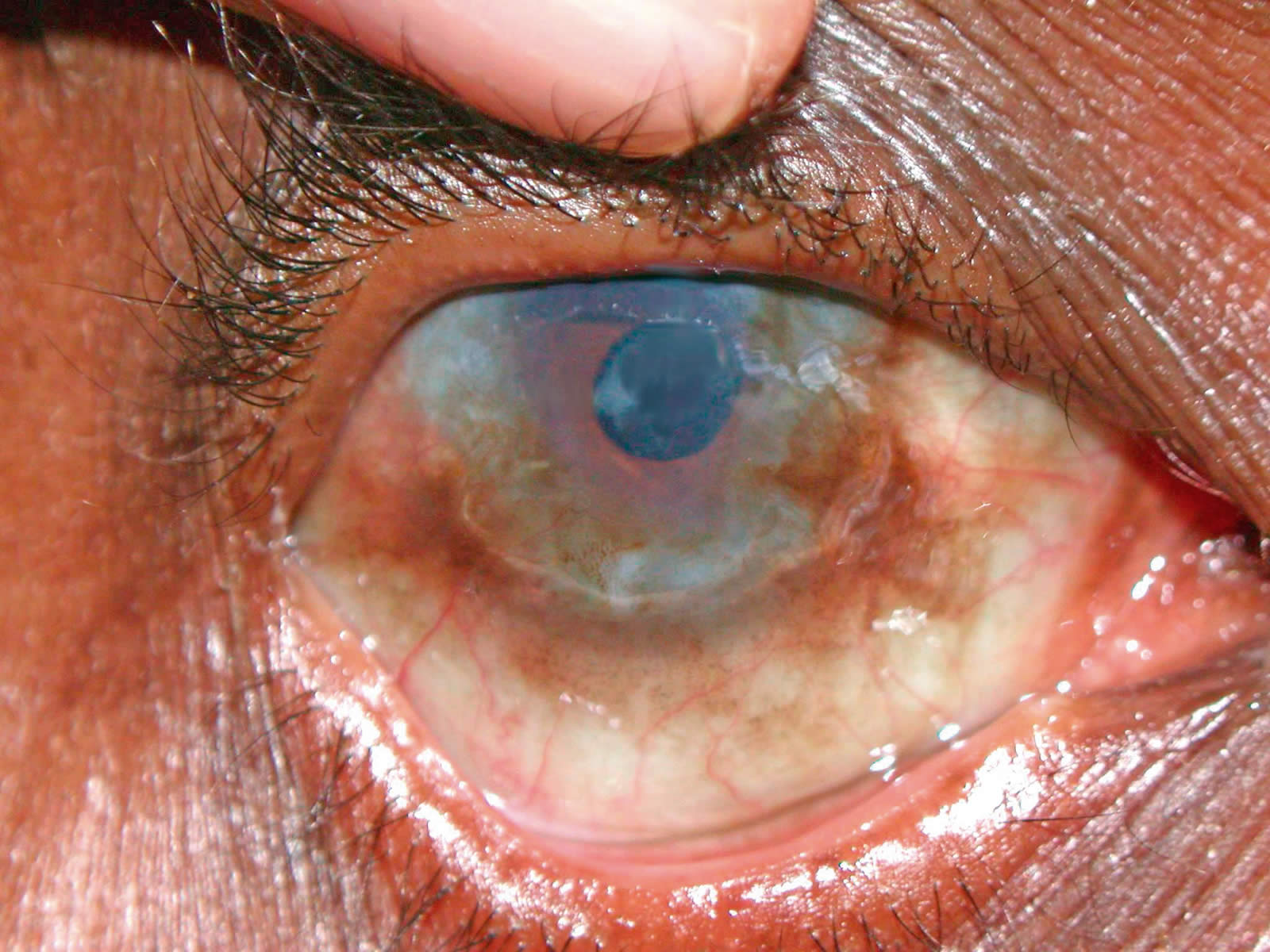
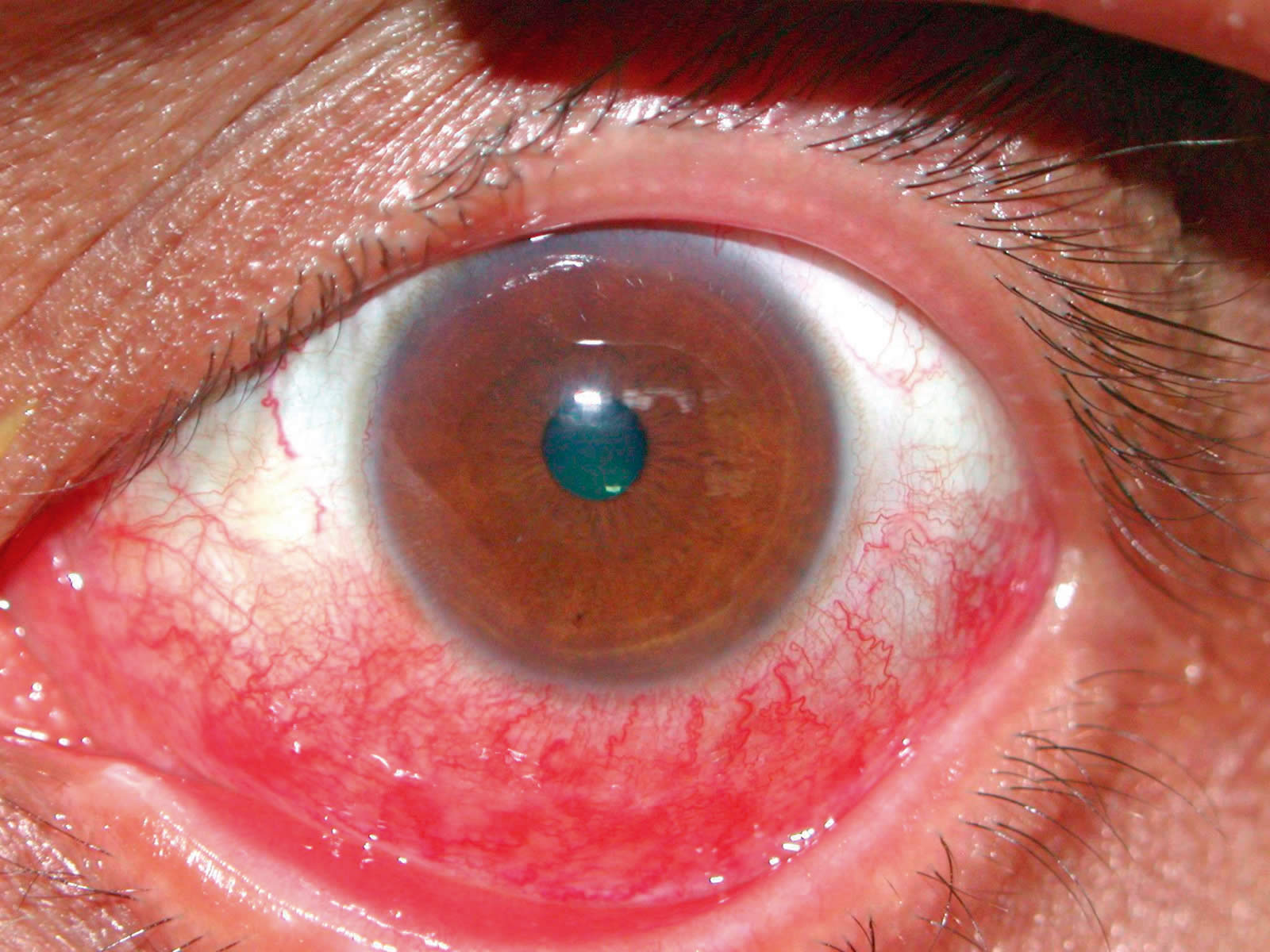
Fig.2. Right eye of patient in Fig.1. Note the dilated, injected conjunctival vessels, Trantas’ dots, and corneal scarring and vascularisation. The white tissue in the nasal portion of the pupil is posterior capsule opacification, following cataract surgery.


A large number of children are affected
Over a quarter of 2,250 children seen at a tertiary referral paediatric eye clinic in East Africa had vernal keratoconjunctivitis. Even more came flocking to screening clinics complaining of itchy eyes.
This is time consuming and frustrating
Typically a child seen with VKC is given one bottle of a mast cell stabiliser and is seen again a few months later apparently no better. Alternatively steroids are used, without a mast cell stabiliser and no counselling about the disease. Quite often children move from one clinic to another picking up another bottle of steroids when the symptoms become unbearable. Both patient and clinicians are frustrated. Over 50% of patients may still have symptoms after five years.1
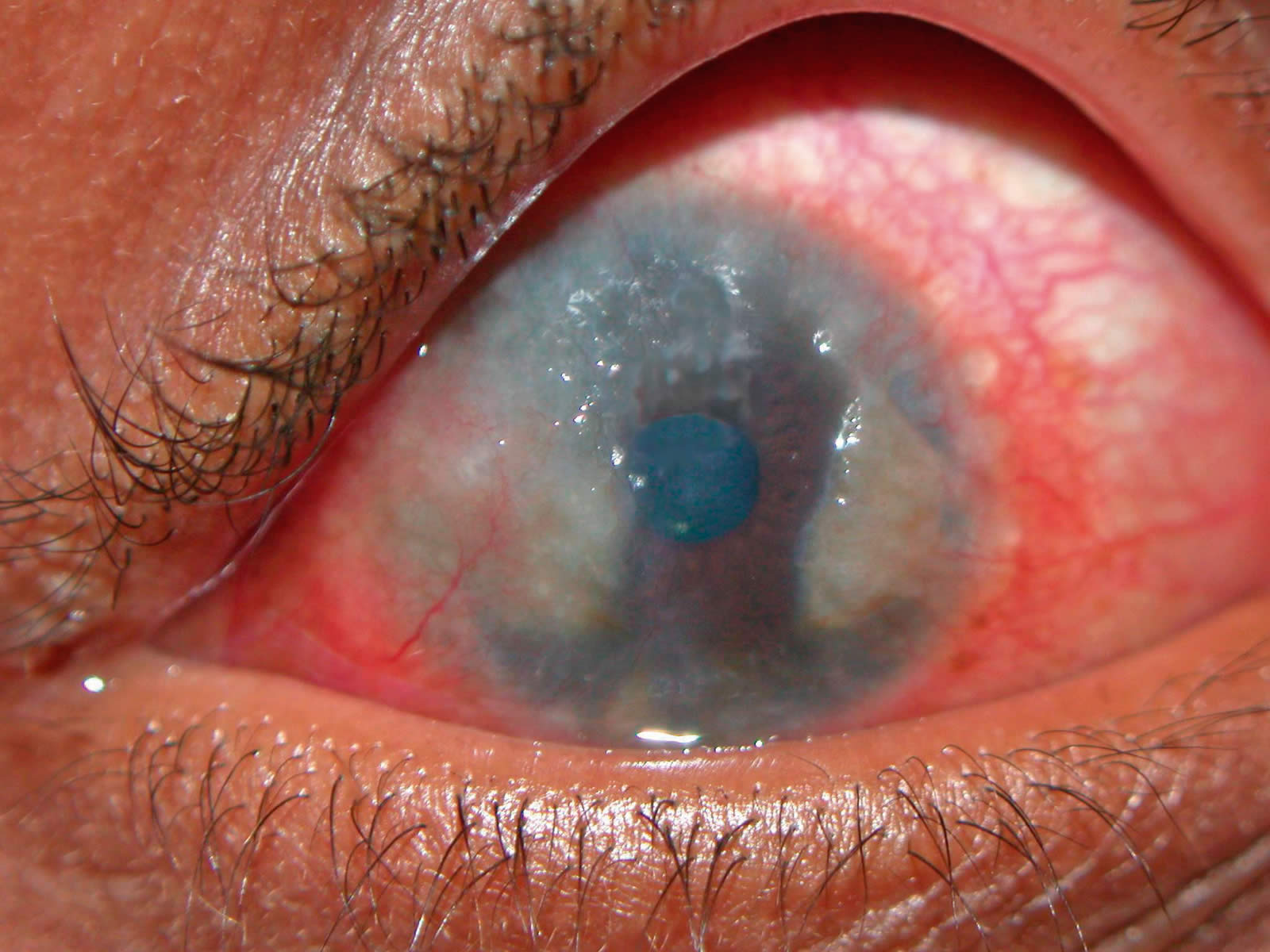
Patients may be blinded by the disease (Figure 4)
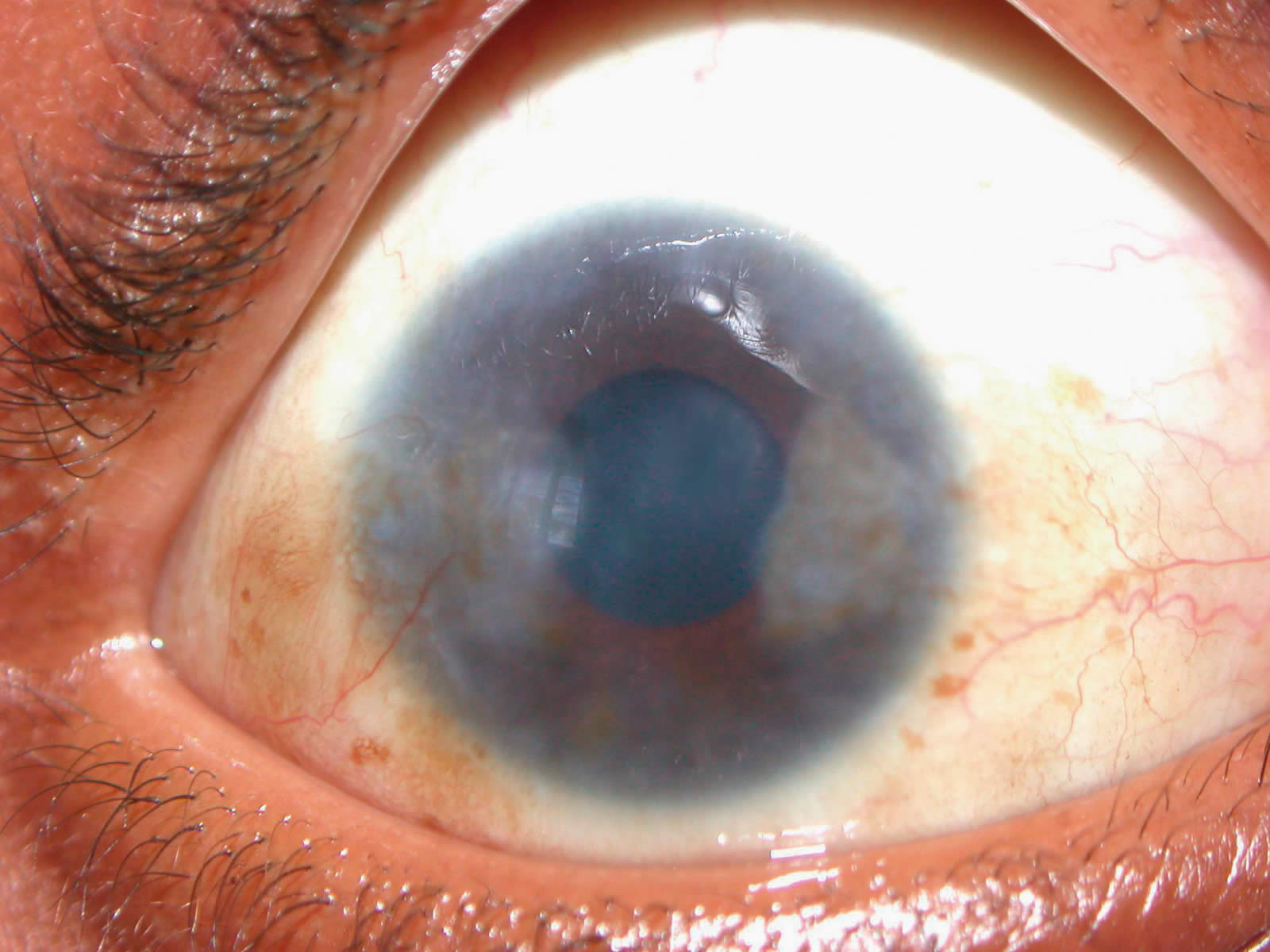
Up to 10% of patients develop corneal ulcers, which may lead to visual loss due to corneal changes. The figure may be higher in hotter climates. Other patients will have visual impairment due to glaucoma and cataract2or extensive cornea pannus (Figure 2 and Figure 6).
How can this frustrating situation be improved?
- By recognising the features of the disease, particularly potentially blinding complications.
- Ensuring that these patients get adequate continuous treatment through good patient education and regular, long-term follow-up.
Recognising the disease: clinical features
VKC is a bilateral chronic inflammation of the conjunctiva. It is more common in young boys. The disease affects children between three to 16 years of age though it may appear earlier than that and continue into adulthood (Figure 1). In the majority of cases, symptoms resolve at puberty. Although the name vernal suggests a seasonal spring time occurrence, frequently the disease persists throughout the year.
Symptoms
Symptoms include intense itching, irritation, photophobia (sensitivity to light) and burning. The itching is worse with exposure to wind, dust, bright light and hot weather. Some patients complain of a sticky, stringy mucous discharge. Corneal involvement leads to complaints of reduced vision.
Signs
In order to elicit the signs, patients should be examined using a slit lamp or magnifying loupes. The use of fluorescein will help to identify sight threatening corneal involvement. The disease is characterised by giant papillae. In the palpebral form, giant, flat-topped papillae of the upper tarsal conjunctiva lead to a clinical picture of ‘cobblestones’. Corneal involvement has been reported in as many as 50% of the patients with the palpebral type of the disease. Corneal involvement may range from superficial punctate keratopathy to shield-like ulcers.2 These may heal leaving a vascularised scar.
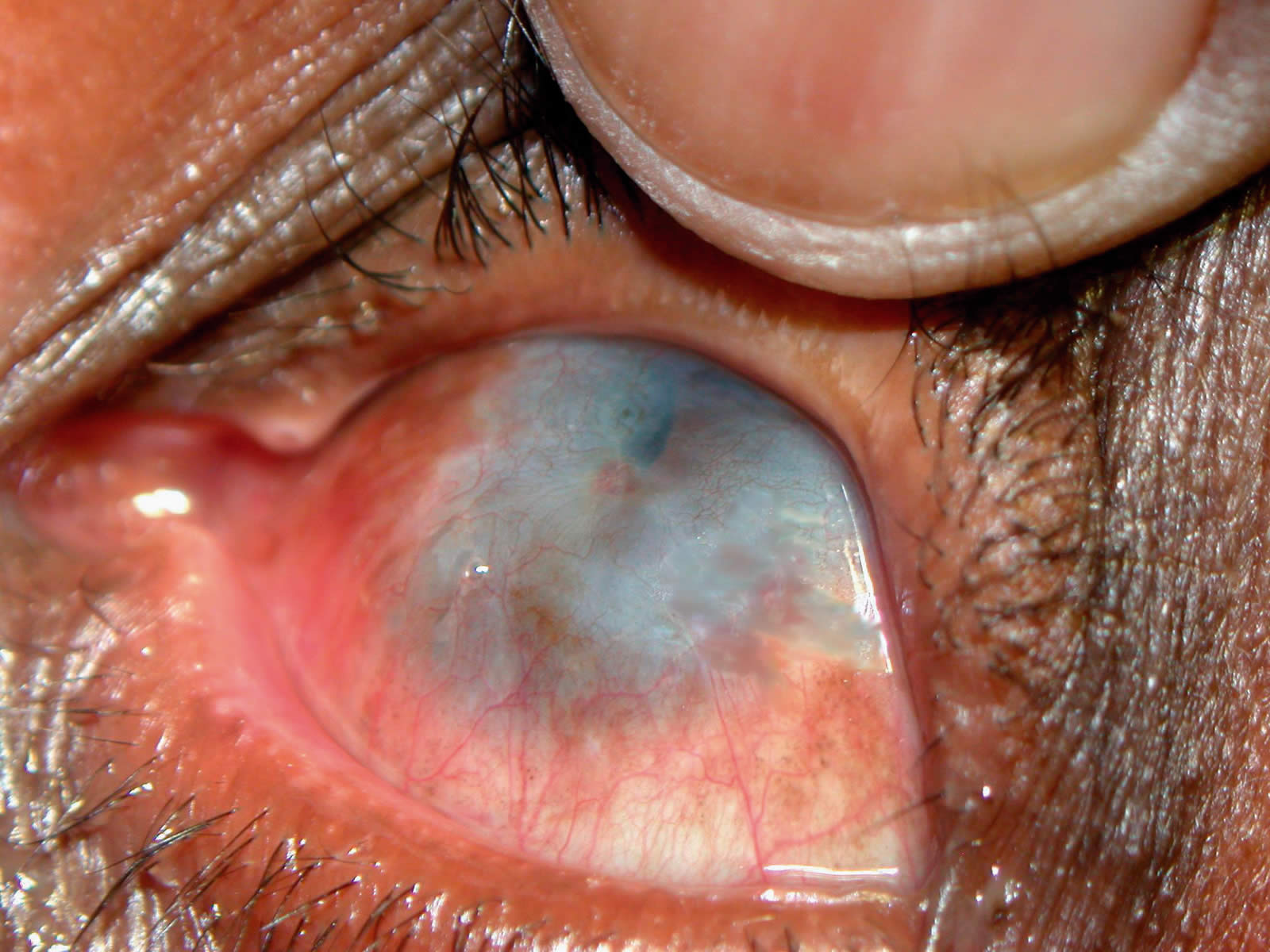
The limbal form is more common in dark-skinned races and females. It is characterised by conjunctival hyperaemia and papillae at the corneal-scleral (limbal) border and Trantas’ dots. The latter are aggregates of epithelial cells and eosinophils. A gelatinous pannus may invade the cornea (Figure 6). Neovascularisation of the cornea may follow (Figure 4). Conjunctival changes include hyperpigmentation (Figure 2), subconjunctival fibrosis, keratinisation and symblepharon.
Visual impairment is more pronounced in cases with shield ulcers and corneal plaques.
The clinician also needs to be constantly on the lookout for the other major complications of cataract and glaucoma especially with prolonged steroid use.
Providing adequate continuous treatment
Counselling
Once the severity of the disease has been characterised, a treatment plan is devised.
We examine and counsel the many children coming to the free district eye clinics in groups. Those with no signs of allergic eye disease are given advice on frequent face washing and cold compresses. They should not be given a bottle of steroid or chromoglycate drops, tempting as this might be. Unnecessary drops can make the situation worse (Figure 7).
Children with signs of allergic eye disease and those presenting to the tertiary referral centre who tend to have more severe disease are examined in more detail and counselled individually. Individual counselling, backed up by patient information leaflets, is critical in breaking the cycle of inadequate treatment and resulting frustration.
Counselling stresses the chronic nature of the disease, that sodium chromoglycate drops take time to work and need to be continued once the child feels better. Children getting steroid drops are told to use these frequently initially. The need to use these for only a short period of time in order to avoid complications is explained. The majority of children and parents respond well to this counselling. As a result, many patients return for review before drops have run out and the symptoms and signs worsened. The use of a dedicated counsellor will save the busy clinician valuable time.


Drug treatment
Treatment is symptomatic and tailored to the severity of the disease.
Those with milder symptoms and no corneal involvement may be given mast cell stabilisers such as sodium chromoglycate or newer agents such as alomide and nedocromil. (If you have access to a low-cost drop manufacturer you can ask for 4% sodium chromoglycate for more severe cases). Topical antihistamines are effective as well.
The mast cell stabilisers must be used regularly three to four times daily, even when there are no symptoms in order to stabilise the mast cells and prevent the release of histamine. They are of no value when used only when symptoms occur because their effect is not immediate. If well used, they can limit or stop the use of steroid drops. They do not have any of the side effects of steroids and can therefore be used for a prolonged period.
Those presenting with corneal involvement and more severe disease should be managed at secondary and tertiary level where they may be given topical steroid drops (e.g. prednisolone, dexamethasone), the most effective available topical medication for severe vernal keratoconjunctivitis. A mast cell stabiliser should be started when the steroids are started. Steroids should be used frequently initially and then tapered to a stop once the acute stage of the disease is stabilised (usually a few weeks). Their use requires monitoring because of the possible effect on intraocular pressure.
Those not responding to conventional treatment may be given supratarsal injection of steroids4 by an eye specialist (Figure 5). Both long-acting steroids such as triamcinalone and shorter-acting steroids (dexamethasone) have been found to be effective in bringing about resolution of the eye signs. Some studies suggest that the recurrence rate of the disease is lower following the use of longer-acting steroids like triamcinolone. Theoretically there is an increased risk of persistent elevation of intraocular pressure with the longer acting steroids. In children, these injections often need to be administered under general anaesthesia. However, with good use of local anaesthesia and careful counselling, children as young as 12 may be safely injected without recourse to general anaesthesia (Figures 8 – 10).
Cyclosporine A drops (0.5-2%) in olive oil or castor oil four times a day are an effective alternative to steroids in severe VKC, if available.3 Cryotherapy of the palpebral conjunctiva may produce additional inflammation with little benefit.2 Debridement of early mucus plaques may speed repair of the persistent epithelial defects. Bandage contact lenses are helpful in the treatment of these defects.
Supportive therapy like artificial tears, cold compresses and sunglasses often help and are commonly overlooked.
Drug allergies
Allergic reaction in the conjunctiva can be provoked by a drug or its preservative. Common drugs include neomycin and gentamicin. These are common in postoperative drops. When examined, the conjunctiva and the lower eyelids will be swollen. The skin may be excoriated. The first measure in the management is to stop using the allergen. Topical steroids may also be used to relieve the symptoms. Far too often the offending drug has been given for a minor symptom because the patient expects drops. This often does more harm than good (Figure 7).
References
1. Bonini S, Bonini S, Schiavone M, Centofanti M, et al. Vernal keratoconjunctivitis revisited: a case series of 195 patients with long-term follow-up. Ophthalmology. 2000;Jun;107(6):1157-63.
2. Bonini S, Coassin M, Aronni S, Lambiase A. Vernal keratoconjunctivitis. Eye 2004;18:345-51.
3. Cameron JA. Shield ulcers and plaques of the cornea in vernal keratoconjunctivitis. Ophthalmology. 1995;102:985-93.
4. Saini JS, Gupta A, Pandey SK, Gupta V, Gupta P. Efficacy of supratarsal dexamethasone versus triamcinalone injection in recalcitrant vernal keratoconjunctivitis. Acta Ophthalmol Scand. 1999;77:515-8.
5. Pucci N, Novembre E, Cianferoni A, et al. Efficacy and safety of cyclosporine eye drops in vernal keratoconjunctivitis. Annal Allergy Asthma Immunol. 2002;89:298-303.
Acknowledgments
The authors are grateful to Dr Amos Kibata for helpful comments on a draft of this manuscript. Dr Debbie Carmichael set up the protocols for effective management of VKC at KCMC and prepared a patient information leaflet.