")
Squamous cell carcinoma in HIV/AIDS
Related content
Epidemiology
Since the 1980s, the number of patients presenting with squamous cell carcinoma of the conjunctiva has been increasing exponentially. 1, 2 In ophthalmic outpatient clinics in Harare, at least two of every one hundred patients have squamous cell carcinoma. The patients vary in age from eighteen to sixty years with the majority between twenty and forty years. Both males and females are affected. Often, the squamous cell carcinoma of the conjunctiva may be the only manifestation in an otherwise healthy looking adult. A large number of ill-looking patients may also present with the conjunctival carcinoma, in addition to other stigmata of immuno-suppression, such as dryness and increased pigmentation of the skin of the face. Some patients have molluscum contagiosum lesions on the lids and forehead
Pathogenesis
The exact cause of squamous cell carcinoma is not known, but the human papilloma virus (HPV) has been implicated. Polymerase chain reaction tests have turned positive in patients with squamous cell carcinoma. It is suggested that the immuno-supression results in co-infection with the papilloma virus. The immuno-suppression causes reduction in the effectiveness of the immune surveillance system resulting in growth of the tumour.
Clinical presentation
Symptoms and signs
The majority of patients complain of a growth in the eye. They may describe a whitish growth which is progressively increasing in size. Often patients experience a foreign body or pricking sensation. In some cases they complain of a red, painful eye. Patients with recurrent squamous cell carcinoma invariably complain of a deep and severe pain around the eye. The pain can be so severe that the patients request enucleation despite good vision. The type of carcinoma seen in our patients is very aggressive.3
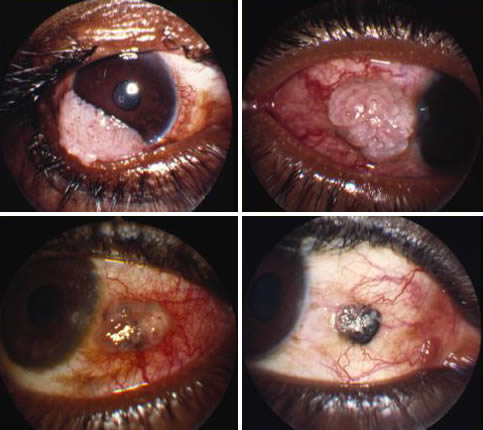
Examination
On examination, these patients have a growth located on the nasal conjunctiva near the limbus or mid-way between the limbus and the caruncle. Typically, the lesion is gelatinous, greyish white on the surface of what appears to be a pingueculum or pterygium. The growths vary in size from 2-3mm, and cover the nasal one third of the cornea. The bigger lesions appear necrotic. While most of these lesions slough off the cornea, some are embedded to underlying sclera. Recurrent tumours tend to be diffuse. We often see tumours invading 2-3mm into the cornea, from 7 o’clock to 10 o’clock. The lateral conjunctiva can be affected, but this is rare.
Differential diagnosis
- Pingueculum
- Pterygium
- Foreign body
- Carcinoma in situ
- Kaposi’s sarcoma
- Lymphoma
In the initial stages, the carcinoma can easily be confused with pingueculum or pterygium. Where HIV is prevalent, it is advised to excise completely suspicious lesions, for biopsy. Carcinoma in situ invariably progresses to squamous cell carcinoma of the conjunctiva. Kaposi’s sarcoma tends to be darker and highly vascularized. In our population these lesions are more likely to be located on the lids, as opposed to the conjunctiva. Lymphoma of the conjunctiva is less common but is typically salmon pink in colour. We perform excision biopsy in all these lesions.
Diagnosis
This is determined by excision biopsy.
Pathology
Histology of these growths typically shows the following features:
- Squamous cell proliferation
- Dyskeratosis
- Acanthosis
- Stromal invasion
- Concentric collection of epithelial and spindle cells.
Management
We strongly recommend excision of any obvious or suspicious lesions after the first visit. Some of these lesions can grow very rapidly. It is important to excise with a margin of at least 2mm of normal looking conjunctiva, as well as remove as much of the base of the tumour as possible. In our experience, most recurrences appear to arise from inadequate removal of the tumour embedded in sclera.
Enucleation is performed routinely in our clinics for recurrent squamous cell carcinoma. This has to be performed on patients who have had several excision biopsies.The bulk of our rural patients are often lost to follow-up, only to present with recurrent tumour which has extensively spread to the fornices.
For those patients where tumour has spread to the fornices and lids, exenteration is the procedure of choice.
Radiotherapy does not appear to be of any help in the management of these patients. Despite local application of radiotherapy to the tumour bed, post-operatively, we have still experienced recurrences.
Chemotherapy, in the form of mitomycin application to the tumour bed, has been suggested to reduce recurrence.We are awaiting our initial results. (See ‘Abstracts’ on page 44 – Editor).
Conclusion
In sub-Saharan Africa, squamous cell carcinoma of the conjunctiva has become a highly significant and blinding condition. Recurrences of the tumour following surgery are becoming more frequent. Tumour development in one eye, following enucleation of the fellow eye for recurrent carcinoma, presents an emotionally difficult challenge for both patient and surgeon. We can only hope, in the short term, that increasing availability of anti-retroviral drugs may reduce the incidence of this disease.
References
1 Muccioli C, Belfort R, Burnier M, Rao N. Squamous cell carcinoma of the conjunctiva in a patient with acquired immune deficiency syndrome. Am J Ophthalmol 1996; 121: 94-96.
2 Margo C E, Mack W, Guffey J M. Squamous cell carcinoma of the conjunctiva and human immunodeficiency virus infection. Arch Ophthalmol 1996; 114: 349.
3 Lewallen S, Shroyer K R, Keyser R B, Liomba G. Aggressive conjunctival squamous cell carcinoma in three young Africans. Arch Ophthalmol 1996; 114: 215-218.