")
Ocular manifestations of child abuse
Related content
Introduction
An old lady takes a grandchild, out of concern and compassion, to a traditional healer for advice and prevention of cataract, a condition the child is likely to develop sixty years later. A concoction of various herbs is prepared and prescribed which subsequently leads to bilateral total damage of the corneae, a disruptive keratomalacia-like reaction. A helpless child, victim of traditional and social practices, enters into a life of almost 50 blind and hopeless years.
It is partly the increased, multifactorial, infant and young child morbidity and mortality that led to the United Nations Convention on the Rights of the Child. This calls for special care and protection of children because of their vulnerability. It states that all countries shall ensure good health for children and protect them from neglect and all forms of exploitation.
In developing countries, children may account for 40-50% of the total population. Yet, they are conspiculously neglected when national eye health and rehabilitation programmes are planned. Most strategies are aimed at the adult group.
The challenge
The challenge lies in a better understanding of the immense eye problems affecting the under-served and vulnerable paediatric group in developing countries and in devising comprehensive national programmes to deal with these problems. It is estimated that childhood blindness causes 90 million blind years (number blind x length of life).
Improved media reporting in recent years has exposed some of the neglect and abuse children are subject to in many societies. However, more information is needed, in particular from Africa. In high-income countries, it is recognised that factors such as broken families, social dysfunction, depression and unemployment play a major role, for instance, in child battering (physical assault of children).
In developing countries, poverty, social and cultural beliefs and taboos and exposure to traditional practices predispose the vulnerable paediatric group to abuse. In many middle- or high-income countries, there is now emergency guidance and advice. Helplines are available whereby children can call for help in the event of abuse. This is still not the case in most low-income countries.
The authors wish to highlight a group of children who, due to well-meant but harmful traditional practices in combination with neglect and sometimes outright abuse, present with ophthalmic manifestations. There is generally a high incidence of eye diseases in children which means that children are particularly at risk of harmful traditional and cultural therapeutic practices.
The leading causes of visual insult in children include:
Traditional eye medicines
Traditional healers instill herbal concoctions into the eyes for trivial complaints. A herbal twig implanted under the eyelid in a child with mild allergic conjunctivitis led to fulminating panophthalmitis (Figure 1). Herbal ocular medicines are responsible for an estimated 8-10% of corneal blindness in Africa. This permanent damage is the result of herbs with a very high pH or the introduction of micro-organisms that can lead to suppurative keratitis and endophthalmitis. Extract of lemon peels are used for serious eye infections, whereas juice from tomato leaves is used for milder conditions.

The most common eye diseases treated in children are allergies, conjunctivitis and trachoma. In the case of trachoma, one healer in Kenya used the rough leaf of .ordia sinesis to rub on the tarsal conjunctiva until it bled. Another chewed the leaves of boscia coreacea, and the juice obtained along with the saliva was applied to the conjunctival sac, a procedure causing irritation, pain and possibly chemical burns. Also observed were cases of gonococcal conjunctivitis among children and these followed instillation by the traditional healer of his own infected urine into the eyes of children presenting with trivial ocular complaints.
Aftermath of drought and famine
Children are the most vulnerable group during droughts and famine. Inadequate nutrition and poor hygiene due to lack of water cause varying degrees of malnutrition and diseases that lead to blindness.
In some communities, already with depleted food supplies, it is customary for adults and children to share a meal around a common plate. The adults reach for the food first and children struggle to reach the plate.
Ocular Injuries and Burns
A nine-day old child of an overburdened and overworked mother, living in a small crowded place, was left by the mother near a kerosine cooking pot. The stove toppled giving the child extensive burns (Figure 2). A number of these cases are accidents in the home such as burns, falls with injury, or even suffocation.

Socio-cultural Attitudes
Many mothers and children, through no fault of their own, are forced to live in over-crowded, unhealthy environments and under marginalised conditions that greatly contribute to trachoma, the second leading cause of blindness in Africa.
Ethnic Conflicts and Wars
Thousands of children are maimed and mutilated in wars and by landmines. A case presented here exemplifies the plight of these children due to man-made disasters and catastrophes (Figure 3).

Sexually-related Abuse
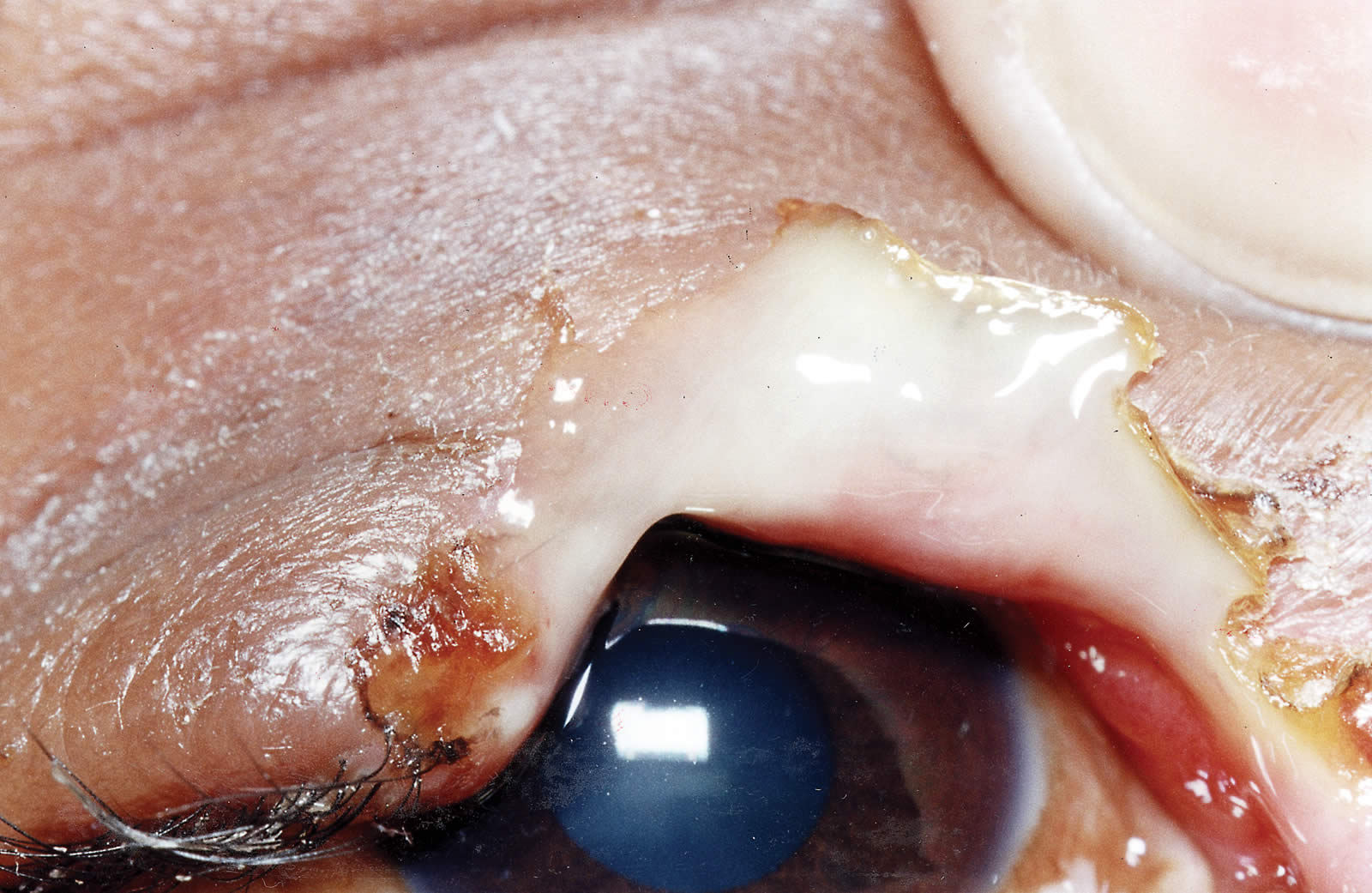
Sexual abuse of children, aged 10-15 years, in low-income countries may be more widespread than is generally thought. In rare instances, such abuse may lead to traumatic eye conditions with serious long-term psychological and physical consequences for the child. A case presented here with a human bite in a 12 years old girl rape victim (Figure 4).
Gonococcal Conjunctivitis
Gonococcal conjunctivitis of the newborn is still a major problem in many countries. We would like to document a 14 months old child with frank gonococcal conjunctivitis (Figure 5) contracted from an infected mother. Sexually transmitted disease and now HIV/AIDS are the scourge of our times. A mother infected with herpes zoster ophthalmicus carries a child (Figure 6).




Social Structures: Womens Rights
A husband is often the only person in a household who gives consent or decides if a child can receive hospital treatment, be it surgical or medical, emergency or otherwise. Often the husband is not readily available. Advanced cases of infected perforations or inoperable retinoblastoma (Figure 7) pose a challenge to the attending ophthalmologist. This may result from experimentation with traditional medicines and later the father may refuse to give his consent for surgical treatment. Parents desperately wanting a male child, deliberately pushed this teenage daughter into a fire (Figure 8).
Squint and Amblyopia
Very rarely have the eye health planners concentrated their strategies on conditions 0ike squint with resultant amblyopia, refractive errors and dyslexia. These condition can lead to major visual impairment, mostly unnoticed by parents and teachers.
Children with such eye problems are scorned and even expelled from school for no fault of their own – by teachers who do not understand the experience and the disability of these children. Sight is precious and essential in the development of the child.
Conclusions
We feel that clear and definite steps should be taken in some developing countries to establish an awareness about the Rights of the Children and to protect them from the negative effects of cultural, traditional and social practices.
The education system is the developing worlds broadest channel for the dissemination of health information, health attitudes and practices. Teachers and leaders can play a major role in promoting the health of children and protecting one of our most essential organs – the eyes.
Greater emphasis must be given to the issue of integrating the traditional healers into primary eye care systems. These first-line providers of health are easily accessible and acceptable to the rural populations and can make a vital contribution at community level in rural areas.
Re-produced with permission from NU Health Care Journal, Sweden 1/97 Volume 11.