")
Managing and treating intraocular retinoblastoma
Related content

In order to improve the survival rates of children with retinoblastoma, a collaborative and multidisciplinary approach is essential, as is a listening ear for parents who may struggle with the difficult decisions facing them
Enucleation remains the mainstay of treatment for advanced intraocular retinoblastoma. This is particularly important in unilateral retinoblastoma in groups C, D and E (Table 1) in low-resource countries, where follow-up may be poor. Acrylic implants and shells/prostheses may cost less than US $10 each and, if available, will ensure that the social and emotional welfare of the child and parents are catered for.
The importance of listening to parents
Doctors who deal with retinoblastoma and enucleation regularly can forget how terrifying it all is for the newly diagnosed family. Taking time to truly listen to parents and address their concerns are an essential part of counselling about treatment and rehabilitation options. Surgery can save a life, but so too can a quiet, listening presence and responsive, empathetic guidance that meets the family in their place of pain and helps them to find a way out of it. The parents of a child whose life has been saved by unilateral enucleation may also be helpful in counselling other families who may think about refusing enucleation due to fear about the outcome.


Multidisciplinary approach
In order to reach – or maintain – high survival rates of over 95%,1 it is essential that there is a collaborative multidisciplinary approach with a trained pathologist and a paediatric oncologist. Otherwise, high-risk features such as massive choroidal invasion and/or retrolaminar optic nerve invasion will not be detected and the child could still die from metastases (secondary spread of the tumour), despite enucleation.
Systemic chemotherapy
This may be given systemically as first line treatment for children with intraocular retinoblastoma in groups B, C and D (Tables 1 and 2), particularly those affected in both eyes. Regular follow-up is essential. If systemic chemotherapy is given, with additional focal therapy (see below), enucleation can be avoided in over 95% of eyes with groups B or C retinoblastoma.
Table 1 Treatment of intraocular retinoblastoma
International Intraocular Retinoblastoma Classification (IIRC)
| Definition | Treatment | |
|---|---|---|
| A | Small tumours <3 mm outside macula | Focal treatment. If no focal treatment available either: Send to a site with focal treatment or if no focal treatment is available in country please seek expert guidance |
| B | Bigger tumours >3 mm or Tumours in the macula or Tumours with sub-retinal fluid | Focal treatment with or without (+/-) systemic chemotherapy up to 6 cycles> |
| C | Localised (within 3 mm from the tumour) vitreous or sub-retinal seeds | Unilateral: Enucleate
Bilateral: Attempt ‘Second Eye’ Salvage: Systemic chemotherapy 6 cycles +/- focal treatment |
| D | Diffuse (> 3 mm away from the tumour)
vitreous or sub-retinal seeds
If Enucleated look for: High Risk Histopathological Features: Retrolaminar optic nerve involvement Choroidal Invasion >3 mm |
Unilateral: Enucleate
Bilateral: Attempt ‘Second Eye’ Salvage: Systemic chemotherapy +/- focal treatment. IF EYE SALVAGE FAILS: enucleation. Post Enucleation: If low risk histopathological features present – no further treatment If high risk histopathological features present: 6 cycles of chemotherapy |
| E | Any of the following:
|
Enucleation.
If low risk – no further treatment.
If high risk histopathological features present (as for Group D): 6 cycles of chemotherapy |
Table 2 Standard dose systemic chemotherapy given every 3 weeks for Intraocular Rb
| Drug | Dose: Mg/m2 | Rate of infusion | Diluent |
|---|---|---|---|
| Vincristine | 1.5 mg/m2 body surface area (BSA D1) (to a max. of 2mg/ dose) | Slowly over 10 minutes | Not less than 10 mls of 0.9% NaCL Note: Risk of extravasation |
| Etopside | 300 mg/m2 BSA D1 | 4-hour infusion | 0.4 mg/ml in 0.9% NaCl Note: Rapid infusion will lead to hypotensive crisis |
| Carboplatin | 600 mg/m2 BSA D1 | 1-hour infusion | 0.5 mg/ml in D5% or DNS |
| Requirements before each cycle |
|---|
| ANC > 1; Platelets > 100; Check that Hb, Renal profile, LFT’s and Magnesium levels are adequate |
| Age | Dose modifications |
|---|---|
| < 6 mth | Give 50% of the dose for each drug |
| 6-12 moths | Give 75% of the dose for each drug |
| 12+ mths | No modification |
Focal therapy
Focal therapy includes transpupillary thermotherapy (TTT), laser photocoagulation, cryotherapy, and plaque radiotherapy. Of these, laser and cryotherapy are likely to be available in low-income countries. All of these can be used either alone (in infants with retinoblastoma identified as being in Group A and possibly Group B), or after initial systemic chemotherapy in Groups B, C & D retinoblastoma. Focal therapy works best for small tumours (less than 5mm), or recurrences with no associated vitreous and/or subretinal seeds.
Laser photocoagulation
Laser treatment is likely to be more readily available than TTT as the laser used for diabetic retinopathy in adults can be modified and used as an indirect laser for treating retinoblastoma. Treatment involves application of argon 532/810 mm laser (above 65 °C) either directly on the tumour, or in a ring-like fashion around it to coagulate the feeding blood vessels, leading to ischaemic tumour damage. In the next 2-3 sessions, the tumour is repeatedly covered with laser burns. Complications include vitreous seeding, vascular occlusions, pre-retinal fibrosis and associated retinal traction and vitreous haemorrhage.
Cryotherapy: Anterior/peripheral small tumours
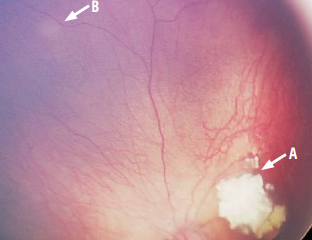
This involves the application of sub-freezing temperatures (down to -90 °C) directly to the tumour mass, resulting in damage to the vascular endothelium with secondary thrombosis and infarction of the tumour. Tumours are typically treated by triple freeze thaw technique through the conjunctiva in two sessions with a 3-weekly interval (Figure 1). Complications include lid oedema, conjunctival chemosis (swelling), serous retinal detachment, vitreous condensation (which can result in vitreous haemorrhage) and tractional retinal detachment.

Plaque therapy: Larger tumours or areas of relapse
Radioactive plaque brachytherapy can be used for tumours with basal diameter and height less than 16 mm and 8 mm respectively. Iodine (I 125) and Ruthenium (Ru 106) radio-isotopes are most commonly used. Gold plaques carrying radio-active seeds are sutured to the base of the tumour, to provide 40 Gray (Gy) to the tumour apex over a period of 2–4 days, and the plaque is then removed. Major complications include cataract, radiation retinopathy or papillopathy, optic neuropathy, scleral necrosis and keratopathy.
External beam radiation therapy
External beam radiation therapy (EBRT) for the treatment of retinoblastoma has decreased drastically due to the increased risk of second non-ocular malignancies, particularly in infants under the age of 12 months who have germline retinoblastoma. However, it does have an important role in children with extraocular retinoblastoma in the orbit (see page 19).
Intravitreal chemotherapy
The vitreous contains no blood vessels, therefore drug concentration from systemic chemotherapy is less effective. Melphalan and topotecan (either singly or in combination) are the chemotherapeutic agents that have been given by direct intravitreal injection.2
Intravitreal injection should not be given:
- if there is tumour at the site of the injection
- if tumour extends to the ciliary body
- if there is a bullous retinal detachment or vitreous haemorrhage which obscures the view of the vitreous and retina.
An ultrasound biomicroscope (UBM) or direct vision may be used before treatment to assess the injection site for tumour.
A small diameter needle must be used (30G or smaller). The site of injection should be 3 mm from the limbus into the pars plana. We suggest using a triple freeze-thaw cryotherapy at the injection site as the needle is withdrawn. The eyeball is then gently jiggled with forceps to distribute the drug evenly throughout the vitreous.
The recommended dose of intravitreal melphalan is 20–30 microgrammes for a maximum of 6 injections over 2–3 months, depending on the distribution and extent of vitreous seeds and response to prior injection. Eye salvage rates have significantly improved as a result of this treatment.
Intra-ophthalmic artery chemotherapy
Although not widely available in low-resource countries, direct treatment of the eye via intra-ophthalmic artery chemotherapy has overtaken the use of EBRT for retinoblastoma once systemic chemotherapy and focal therapies have been exhausted. This treatment should be used with caution as first-line treatment for unilateral advanced retinoblastoma (Groups D and E) as they may metastasise. This is particularly relevant if follow-up is poor.

References
1 Kaliki S, Srinivasan V, Gupta A et al. Clinical feature predictive of high-risk retinoblastoma in 403 Asian Indian patients: a case-control study. Ophthalmic 2015;122: 1165-72.
2 Smith SJ, Smith BD. Evaluating the risk of extraocular tumur spread following intravitreal injection therapy for retinoblastoma: a systematic review. Br J Ophthalmic 2013;97(10):1231-6.
With thanks to Abby White of World Eye Cancer Hope for her contribution on counselling parents. www.wechope.org
© The author/s and Community Eye Health Journal 2018. This is an Open Access article distributed under the Creative Commons Attribution Non-Commercial License.