")
Diabetes in adults is now a third world problem*
Related content
* This article first appeared, in unabridged form, in the Bulletin of the World Health Organization, 1991; 69:643-648.
For many years, diabetes mellitus in adults (in its non insulin-dependent form) was considered a disease which afflicted the affluent and resulted from an overindulgent life-style. For this reason diabetes, as well as certain cardiovascular diseases, cancer and other noncommunicable diseases, were thought to be largely a problem of the industrialized nations.
In the past few years, several reports have been published indicating a high prevalence of diabetes in communities in the developing world, and in ethnic minorities in industrialized countries. These include such diverse groups as indigenous Americans,1 Pacific islanders,2 and migrant Asian Indians.3,4 A problem with the earliest reports was the fact that the criteria for the diagnosis and classification of diabetes were not uniform, resulting in a lack of comparability of such studies. It is only in the past 12 years that these aspects have been standardized, thanks to the efforts of the US National Diabetes Data Group3 and the World Health Organization.6,7
Following these important developments in diabetes epidemiology, the published studies that conformed to current WHO criteria for classification and diagnosis were reviewed.8 Recently, the diabetes programme at WHO Headquarters, Geneva, has been collating data from many studies, both published and unpublished, in which the diagnosis of diabetes was based upon the current WHO diagnostic criteria.7 Between 1988 and 1991, all investigators who were considered to have examined diabetes prevalences in unbiased adult population samples, using the WHO diagnostic criteria for glucose intolerance (based on blood glucose measurements two hours after a 75 g oral glucose challenge), were encouraged to submit their data for inclusion in the study. Suitable material was obtained in this way for over 70 populations in over 30 countries worldwide, the total study sample being over 150,000 subjects.
In order to enhance comparability, the prevalence rates were standardized for age in a truncated age range of 30-64 years. The world population described by Segi9 was taken as the standard. Full details of the standardization procedure and detailed results for all populations are published separately.10The present article gives data from selected populations in all WHO regions on the global prevalences of diabetes, and focuses on the pattern in the developing world.
Prevalence data
Diabetes mellitus
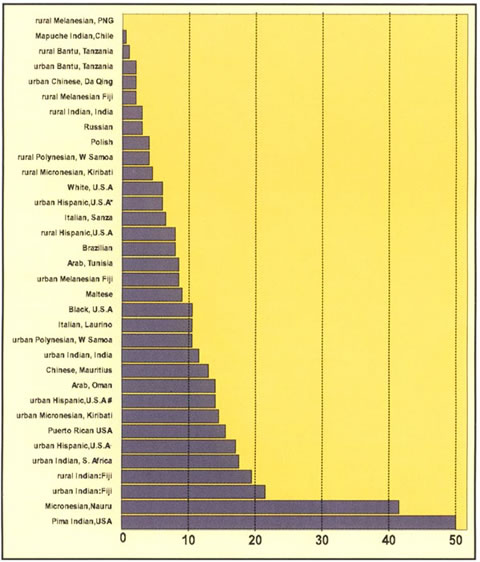
In African and Asian populations, diabetes was rare (1%) among the Tanzanian rural Bantu (Fig. 1). Diabetes was also rare in Da Qing in China – despite the fact that this is an industrial city – and in rural India. Prevalence was close to 10% among Tunisian Arabs, 14% in Omanis, and was of the order of 10-20% among migrant Indian populations (in rural as well as urban locations). The prevalence exceeded 10% among the Chinese Mauritians.
In American populations, prevalence was lowest (<1%) in the rural Mapuche Indians of Chile. In the USA, as compared with a prevalence of 5-7% among whites, the blacks had higher risk (c. 10%); Among US Hispanics the prevalence was approximately 10-20%, and was inversely related to average income in the Hispanic residents of San Antonio. In the Pima Indians diabetes reached the extreme prevalence of 50% in this age range (30-64 years).
In European populations the prevalence was generally lower, ranging from 2-4% in Siberian Russians to 10% in Italy and Malta.
In Pacific populations the prevalence was highly variable. Diabetes was not recorded in a small highland population sample in Papua New Guinea and prevalence was low in rural Fijian Melanesians (unlike their Indian counterparts). Moderate rates were observed in urban Melanesians and in Polynesians. Rates were higher among urbanized Micronesians and in the Nauruans extremely high rates (>40%), close to those of the Pimas, were observed.
In Figure 1, these populations are ranked according to increasing prevalence of diabetes, which can be seen to vary from 0 to 50% in this age range. One most interesting and important observation is that if one takes an arbitrary cut-off point of 10%, above which diabetes in adults can be considered common, it is only among the populations of developing countries, and migrant and minority communities in industrialized countries, that this limit is exceeded.
Impaired glucose tolerance
The category of ‘impaired glucose tolerance’ (IGT) describes individuals whose blood glucose after the oral glucose challenge is above the normal range, but is still lower than that used to define diabetes.5-7 Longitudinal studies suggest that approximately one-third of subjects with impaired glucose tolerance progress to diabetes, and that they are at increased risk of related complications such as cardiovascular disease.11,12
Results of population studies on Impaired Glucose Tolerance and Total Glucose Intolerance may be found in the following original articles by the same authors on behalf of the WHO Ad Hoc Reporting Group:
Diabetes in adults is now a Third World problem. WHO Bull 1991; 69: 643-8.
Global estimates for prevalence of diabetes mellitus and impaired glucose tolerance in adults. Diabetes Care 1993; 16: 157-77.
Total glucose intolerance
Since IGT indicates a high risk of subsequent diabetes and associated disorders such as cardiovascular disease, the combined prevalence of diabetes and IGT (together recording the ‘total glucose intolerance’) is a useful measure of the public health impact of glucose intolerance in a given population.
Implications of the global diabetes data
The standardized information presented in this review demonstrates convincingly that diabetes is a global problem, and also that it reaches its greatest frequency in the developing countries, and among minority groups and the disadvantaged in the industrialized countries. Contrary to traditional belief, diabetes in adults should now be recognized as a particular threat to the public health of Third World communities – those living in the developing countries, as well as the disadvantaged minorities in industrialized nations.
The wide range in prevalence of diabetes, from 0% to 50% in adults aged 30-64 years, is probably greater than that for any other chronic disease and is a strong indication of the importance of environmental factors in the aetiology of non insulin-dependent diabetes (NIDDM). A recent study of approximately 250,000 subjects in 19 Chinese provinces, conducted in 1994, indicated that the prevalence of diabetes is now almost three times higher than it was 10 years ago (Pan Xiao-ren, personal communication).
Since environmental and behavioural factors may be amenable to change, the identification of risk factors for diabetes in all populations should be considered a priority. There is a consistent association between diabetes and urban living, and, for example, amongst US Hispanics in San Antonio, an inverse relationship to income, which suggests the presence of potentially avoidable life-style factors among the disadvantaged.
Inappropriate diet (high content of fat and refined carbohydrate), sedentary lifestyle, and obesity have often been incriminated as the principal environmental determinants of non insulin-dependent diabetes. However, it is still not clear how such factors operate, and if their influence varies between populations.13 The distribution of risk factors within communities is also of some interest in defining strategies for prevention. If risk factors cluster in certain individuals, a high-risk prevention strategy may be very effective; but if they are widely spread among the population, greater emphasis may be given to a population approach.14
Diabetes is a very costly disorder, both to health agencies, in terms of provision of additional services, and also to diabetic individuals and their families, in terms of loss of productivity and reduced quality of life.15 However, it is thought that many of the complications of diabetes may be delayed or even prevented by prompt and effective treatment and education.
Diabetes mellitus is associated with damage to the small blood vessels in the retina, resulting in loss of vision. In economically developed societies, it is a major cause of visual disability in people aged 25 years or older. In Wisconsin, United States of America, in 1980-1982, after 15 years of diabetes, 21% of diabetic people had visual impairment and 6% were legally classified as blind16 In Denmark, blindness or severe visual impairment developed in about 33% of a cohort of younger-onset insulin-dependent (IDDM) people with diabetes followed for 40 or more years.17
More recently, the overall 4-year incidence of visual impairment (9%) and blindness (2%) was estimated in IDDM patients in Wisconsin.18 The 4-year incidence of blindness was higher (3%) in older-onset than in younger-onset IDDM patients (1.5%). As the former are more numerous, they made up a higher proportion (89%) of those who became blind than did the younger-onset group (11%). In the younger-onset group, diabetic retinopathy was the underlying cause of blindness in 86% of eyes; in the older-onset group, blindness was due to diabetic retinopathy in 35% of eyes while in the remainder the causes included cataract, glaucoma and age-related macular degeneration.
Almost everyone with younger-onset diabetes will develop diabetic retinopathy after 20 years of the disease.19 At some time during their lives, 75% will develop the most severe stage, proliferative diabetic retinopathy; in older-onset NIDDM, almost 60% will develop diabetic retinopathy and at some time during their lives about 10% will develop proliferative retinopathy. Both younger- and older-onset diabetic people are at risk of developing another sight-threatening manifestation of diabetic retinopathy, namely macular oedema.
Global surveillance and programmes for primary, secondary and tertiary prevention of diabetes are required. Aware of the modern threat of diabetes to global public health, the Forty-second World Health Assembly adopted a resolution on the prevention and control of diabetes in 1989.20 It invited countries to assess the national importance of diabetes, to implement population-based measures for its prevention and control, and to share opportunities for training and further education.
WHO has prepared guidelines for the development of national programmes for diabetes to assist Member States in this process.21 Most recently, WHO regional offices have begun to establish regional diabetes task forces, reach regional consensus on diabetes care, promote national diabetes programmes, organize training and education and produce guidelines on diabetes management and education.
Epidemic of adult diabetes mellitus
Since 1988, WHO has been collecting standardized information on the prevalence of diabetes and impaired glucose tolerance (IGT) in adult communities worldwide. Within the age range 30-64 years, diabetes and IGT were found to be absent or rare in some traditional communities in Melanesia, East Africa and South America. In communities of European origin, the prevalence of diabetes and IGT were in the range of 3-10% and 3-15% respectively, but migrant Indian, Chinese and Hispanic American groups were at higher risk (15-20%). The highest risk was found in the Pima Indians of Arizona and in the urbanized Micronesians of Nauru, where up to one-half of the population in the age range 30-64 years had diabetes.
The prevalence of total glucose intolerance (diabetes and IGT combined) was greater than 10% in almost all populations, and was within the range 11-20% for European and United States (US) white populations. However, the prevalence of total glucose intolerance reached almost 30% in Arab Omanis and in US blacks and affected one-third of all adult Chinese Mauritians, migrant Indians, urban Micronesians and lower income urban US Hispanics. In Nauruans and Pima Indians, approximately two-thirds of all adults in the age range were affected.
These results lead to three important conclusions. (1) An apparent epidemic of diabetes has occurred – or is occurring – in adult people throughout the world. (2) This trend appears to be strongly related to life-style and socioeconomic change. (3) It is the populations in developing countries, and the minority or disadvantaged communities in the industrialized countries who now face the greatest risk. Diabetes in adults should now be considered not only as a disease of industrialized countries, but also as a Third World problem. All countries should be encouraged to develop national policies and programmes for the prevention and control of this costly disease.
Hilary King and Marian Rewers on behalf of the WHO Ad Hoc Diabetes Reporting Group.
References
1 Knowler WC, et al. Diabetes incidence and prevalence in Pima Indians: a 19-fold greater incidence than in Rochester, Minnesota. Am J Epidemiol 1978; 108: 497-505.
2 Zimmet P, et al. The high prevalence of diabetes mellitus, impaired glucose tolerance and diabetic retinopathy in Nauru – the 1982 survey. Diabetes Res 1984; 1: 13-8.
3 Zimmet P, et al. Prevalence of diabetes and impaired glucose tolerance in the biracial (Melanesian and Indian) population of Fiji: a rural-urban comparison. Am J Epidemiol 1983; 118: 673-88.
4 Dowse DG, et al. High prevalence of NIDDM and impaired glucose tolerance in Indian, Creole and Chinese Mauritians. Diabetes 1990; 39: 390-6.
5 National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979; 28: 1039-57.
6 WHO Technical Report Series No.646. WHO Expert Committee on Diabetes Mellitus: second report 1980.
7 WHO Technical Report Series, No.727. Diabetes mellitus: report of a WHO Study Croup 1985.
8 King H, Zimmet P. Trends in the incidence and prevalence of diabetes: noninsulin-dependent diabetes mellitus. World Health Statistics Quarterly 1988; 41: 190-6.
9 Segi M. Cancer mortality for selected sites in 24 countries (1950-57). Sendai, Tohuku University School of Medicine, 1960.
10 WHO Ad Hoc Diabetes Reporting Group. Global estimates for prevalence of diabetes and impaired glucose tolerance in adults. Diabetes Care 1993; 16: 157-77.
11 Fuller JH, et al. Coronary-heart-disease risk and impaired glucose tolerance: the Whitehall Study. Lancet 1980; 1: 1373-6.
12 Saad MF, et al. The natural history of impaired glucose tolerance in the Pima Indians. New Engl J Med 1988; 319: 1500-6.
13 King H. Aetiology. In: Nattrass M, Hale PJ, eds. Noninsulin-dependent Diabetes. (Bailliere’s Clinical Endocrinology and Metabolism, Vol.2). 1988: 291-305.
14 King H, Dowd JE. Primary prevention of Type 2 (noninsulin-dependent diabetes mellitus. Diabetologia 1990; 33: 3-8.
15 Huse DM, et al. The economic cost of noninsulin-dependent diabetes mellitus. J Am Med Assoc 1989; 262: 2708-13.
16 Klein R, Klein BEK. Vision disorders in diabetes. In: Hamman R, Harris MWH, eds. Diabetes in America, Chapter 13. Bethesda MD: National Institute of Health, 1983: 1-36 (US Public Health Service NIH Publication No.85-1468).
17 Borch-Johansen K. The prognosis of insulin-dependent diabetes mellitus. An epidemiological approach. Dan Med Bull 1989; 36: 336-48.
18 Moss SE, Klein R, Klein BEK. The incidence of vision loss in a diabetic population. Ophthalmology 1988; 95: 1340-8.
19 Klein R. The epidemiology of diabetic retinopathy. In: Williams G, Pickup J, eds. Textbook of Diabetes. London: Blackwells, 1991:2: 537-563.
20 World Health Organization. World Health Assembly Resolution 42.36, (Prevention and control of diabetes mellitus). In: Handbook of Resolutions Vol.III (1985-1989). 2nd edn. Geneva: WHO, 1990:71.
21 Reiber G, King H. Guidelines for the development of a national programme for diabetes mellitus. Geneva: WHO, 1991.