")
Understanding and managing pterygium
Related content
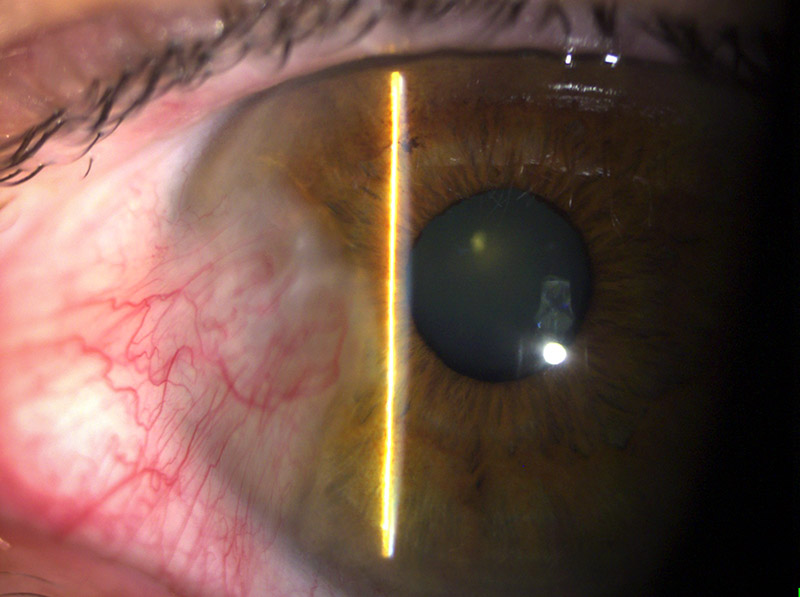
A pterygium is a wing-shaped fibrovascular proliferation of the conjunctiva that grows across the cornea.1 Pterygium occurs more frequently in people who live in areas with high ultraviolet radiation. Dusty, hot, dry, windy, and smoky environments also play a part.2 Most occur on the nasal side.
Diagnosis
Step 1. Taking a detailed history
How long has the growth been present? Typically, this would be for many months or years. This helps to differentiate it from ocular surface squamous neoplasia (OSSN), which tends to have a shorter history (see pages 52–53).
Ask the patient if it has been getting bigger. Some pterygia are inactive and have not grown for decades.
What symptoms is the patient complaining of? There may be redness, irritation, blurring of vision, double vision, itching, and a concern about the cosmetic appearance.3
Step 2: Examination
Check the visual acuity. You should always do a complete eye examination and look for other causes of discomfort or vision loss. Measure the size of the pterygium from the limbus to the apex of the pterygium on the cornea. Record this on a diagram in the clinical record so that, the next time you see the patient, you can tell if the pterygium has grown.
Look for any atypical features that might make you worry about dysplasia (early-stage cancer), such as leucoplakia (an elevated, white, dry-looking patch), a raised gelatinous mass, or a large, prominent feeder blood vessel. Be especially alert if you live in Africa where there is a high prevalence of OSSN.4
Examine the eye movements to look for any evidence of restricted movement caused by the pterygium.
Retinoscopy will reveal any with-the-rule astigmatism that may be caused by the pterygium. Corneal topography can be valuable in detecting irregular astigmatism and distortion caused or induced by pterygium.
When to treat
The most important indications for treatment are:
- Involvement of, or threat to, the visual axis
- Loss of vision from astigmatism
- Restriction of eye movement
- Atypical appearance suggesting dysplasia
- Increasing size (documented by an ophthalmologist)
Less important indications are:
- Increasing size (reported by the patient)
- Symptoms of irritation and complaints of redness, etc.
- Cosmetic issues
Counselling patients
Patients benefit from counselling before and after the operation.
Not every pterygium needs to be operated on. Some patients may expect to have their pterygium removed when simple conservative treatments such as lubricating drops or steroids may be all that is needed. It is important to explain to patients that there is a chance of recurrence, so that the pterygium may come back even if it has been surgically removed. However, surgery with a conjunctival graft (as described opposite) substantially reduces the risk of recurrence.
Compile a list of indications to suit your setting. Use the list to counsel patients about their suitability for an operation. Review them in a few months to see if the symptoms have improved with conservative treatment and to check if the pterygium has grown.
Use an information leaflet to help you to counsel patients. We use a leaflet which has a picture of a pterygium, a list of indications, a description of the procedure, what to expect in the post-operative period, possible complications, and the likelihood of recurrence. The picture is useful in helping you to explain the diagnosis, the indications for surgery and the pterygium operation. Warn patients that the eye may be quite painful for a day or two.
Complications
Patients need to be fully informed about possible complications before you start. Complications can occur during the operation or may present later.
Intraoperative complications include:
- Perforation of the globe
- Thinning of sclera or cornea from dissection
- Intraoperative bleeding
- Excessive cautery
- Muscle damage
- Reversing the conjunctival autograft (placing it epithelial surface down)
Early postoperative complications include:
- Persistent epithelial defects
- Dellen formation (an area of corneal thinning adjacent to limbal swelling that prevents normal wetting of the corneal surface)
- Haematoma beneath the graft
- Loss of the graft
- Pyogenic granuloma
Late complications include:
- Recurrence
- Corneo-scleral necrosis
- Scleritis
- Endophthalmitis
Recurrence is a major late complication. The highest rate of recurrence occurs in the bare sclera technique. 1,5 The section opposite describes a technique of excision with conjunctival autografting, which reduces the recurrence rate.1You may wish to consider using adjuvants such as 5-fluorouracil or mitomycin C, but be aware that mitomycin C is associated with a higher rate of visually threatening complications. Adjuvants can be reserved for recurrent cases.1
Pterygium surgery: the conjunctival autographing technique
Before the operation
Consider using steroids for a few days preoperatively to reduce inflammation.
Before you begin giving the anaesthetic, check the notes to make sure you are proceeding on the correct eye. Mark the eye, as you would for any eye procedure, to avoid possible confusion.
Give the patient topical anaesthetic drops before they come into the theatre. Dilating drops will help reduce the pain from postoperative ciliary spasm.5
Anaesthesia
If you have a cooperative patient, you can infiltrate local anaesthetic under the conjunctiva using a fine-gauge needle. Use a long-acting anaesthetic such as bupivacaine as this can give some hours of pain relief after the operation. Adrenaline will aid haemostasis.
Infiltrate the anaesthetic under the pterygium and under the conjunctival epithelium supero-temporally. The advantage of local in ltration is that the patient retains the ability to move the eye and can be asked to look left, right or down to expose the part of the eye that is being operated on.
Give a sub-Tenon’s anaesthetic if the patient is likely to be uncooperative or if you anticipate a lengthy procedure.
You will need to reassure the patient and explain each step as you proceed with the anaesthesia and the excision.
Pterygium excision and autoconjunctival graft
Pterygium surgery should not be delegated to the most junior trainee surgeon. Supervision of trainees should be continued until they are competent at all the steps required. This will reduce recurrence rates.3
Prepare the patient as you would for intraocular surgery. Wear a sterile gown and gloves, disinfect the skin around the eye and thconjunctival sac with 5% (aqueous) povidone iodine solution, and drape the patient. A scrub nurse should assist you. A surgical pack containing an eyelid speculum, two pairs of Moorfield’s forceps, fine-toothed forceps, Wescott scissors, needle holder, crescent blade or No. 15 blade, bipolar or ball cautery, fine absorbable suture (7-0 or 9-0) or 10-0 nylon and swabs.
Even if you have given a sub-Tenon’s block, injecting anaesthetic with adrenaline under the conjunctiva will help to elevate the pterygium off the sclera and separate the conjunctival epithelium from the underlying Tenon’s capsule.
The vasoconstrictive effect will also limit bleeding. A traction suture may be needed to move the eye if the patient has had a block. This may be inserted through the superior peri-limbal conjunctival tissues or be a corneal traction suture.
Excising the pterygium
To get a good view, ask the patient to look in the direction away from the pterygium.
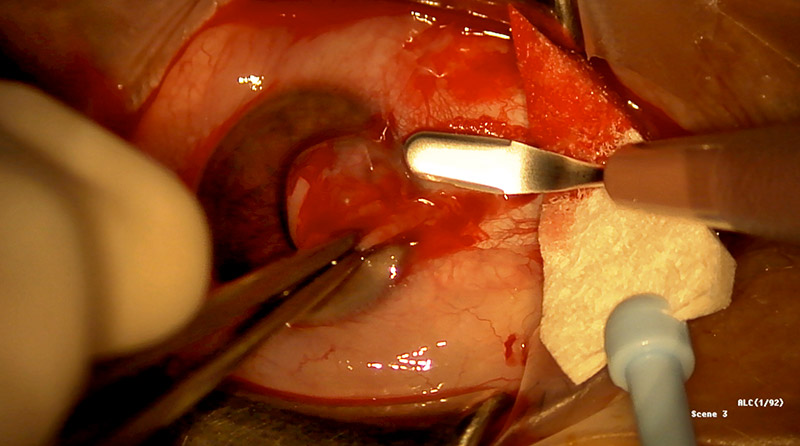
Start the excision of the pterygium by grasping it with Moorfields forceps and making radial incisions with Wescott scissors along the edges. Find the plane under the pterygium and Tenon’s capsule anterior to the medial rectus muscle. Take care to stay away from the medial rectus muscle so that it is not cut or damaged inadvertently. Cut along the base of the pterygium (parallel to the limbus). Make sure you stay anterior to the plica. The pterygium should lift easily off the sclera. It becomes adherent at the limbus and you will need to use a crescent blade or No. 15 blade to carefully dissect it off the cornea (Figure 1). The sclera must be clean of any Tenon’s capsule. Ask your assistant to keep the field free of blood so that you have a clear view of the depth of your dissection. Most bleeding will stop of its own accord. Only use cautery if the bleeding is so profuse that it is likely to form a large haematoma and lift the conjunctival graft off the sclera. A little blood will act as autologous fibrin glue.
Taking the conjunctival autograft
Ask the patient to look down. Marking the epithelium with a sterile skin marker will help you to identify the surface of the graft. Make two radial incisions in the superior bulbar conjunctiva. The incisions should outline an area that is about the same in size as the nasal conjunctival defect. Carefully dissect the conjunctiva off the underlying Tenon’s capsule (Figure 2). Once you are in the correct plane you should incise the conjunctival graft along its posterior edge. Lift the posterior edge and carefully dissect off any adherent Tenon’s capsule. Your assistant may hold one corner of the graft for you. The graft may be placed epithelium up on a paper template (suture cover) before it is cut off from the limbus. This improves the handling and orientation of the thin conjunctival tissue.2
Placing and suturing the graft
Orientate the graft with the limbal donor edge closest to the nasal limbus. Fibrin glue can speed up pterygium surgery and may reduce postoperative pain.2However, the cost of fibrin glue is prohibitive, even in some high-resource settings. A good alternative is 9-0 or 10-0 nylon: it is widely available, cheap, and causes no tissue reaction.5
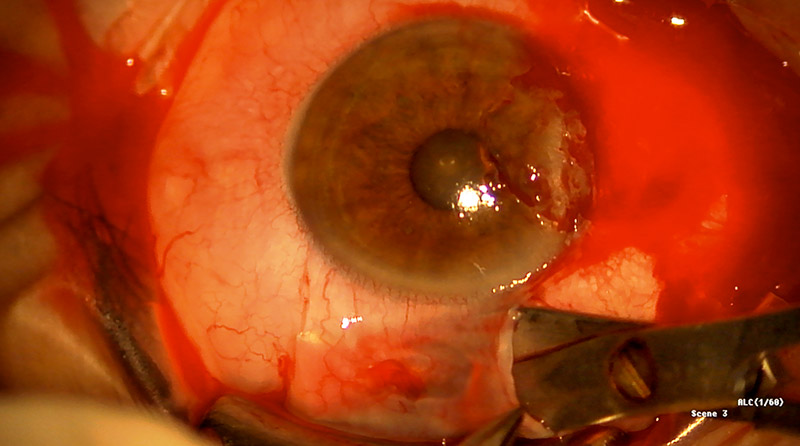
Anchor the two limbal corners to the sclera to avoid posterior migration of the graft (Figure 3). Suture the remaining corners of the graft to the nasal conjunctiva. If you are using nylon, use a mattress suture to bury the knots. Place additional sutures as required to close any gaps between the graft and the nasal conjunctiva.
Apply chloramphenicol ointment to the conjunctiva and firmly pad the eye.
Postoperative care
The patient will need good pain relief after surgery. We prescribe a combination of paracetamol and codeine for a day or two. Ask the patient to install steroid and antibiotic drops 4 times a day for a week. The topical steroid should continue for at least a month. Examine the patient the next day to make sure that the graft is in place.
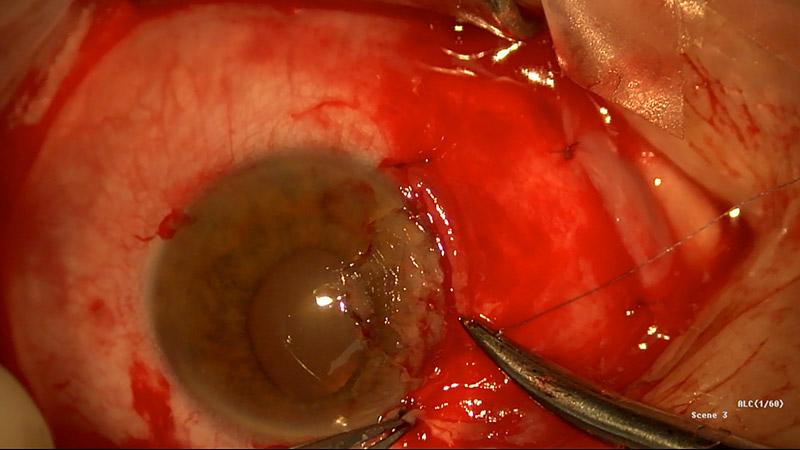
The next visit is at 1 week (Figure 4). Review the patient at 1 month and 3 months to make sure there are no complications. Signs and symptoms of recurrence usually occur 4–6 weeks after surgery.5
Encourage the patient to return in a year so that you can check for any recurrence of the pterygium.
References
1 Kaufman SC, Jacobs DS, Lee WB, Deng SX, Rosenblatt MI, Shtein RM. Options and adjuvants in surgery for pterygium: a report by the American Academy of Ophthalmology. Ophthalmol 2013;120(1):201-8. Epub 2012/10/16.
2 Koranyi G, Seregard S, Kopp ED. Cut and paste: a no suture, small incision approach to pterygium surgery. Br J Ophthalmol. 2004;88(7):911-4. Epub 2004/06/19.
3 Hirst LW. The treatment of pterygium. Surv Ophthalmol. 2003;48(2):145-80. Epub 2003/04/11.
4 Gichuhi S, Sagoo MS, Weiss HA, Burton MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health. 2013;18(12):1424-43. Epub 2013/11/19.
5 Sheppard JD, Mansur A, Comstock TL, Hovanesian JA. An update on the surgical management of pterygium and the role of loteprednol etabonate ointment. Clin Ophthalmol. 2014;8:1105-18. Epub 2014/06/27.