")
The red eye – first aid at the primary level
Related content
The red eye forms a big proportion of the eye problems seen in most eye clinics in developing countries. For example, in the Bawku Hospital eye unit, Ghana, in 2004 a total of 21,391 patients were seen as outpatients, out of which 8,931 were red eyes of one type or another, representing over 40% of the total number of patients screened.
The majority of red eyes are seen at community clinics and health centres, where diagnosis and management are done by community health nurses, primary eye care workers and ophthalmic nurses. It is for this reason that adequate attention should be given to the prevention, early diagnosis and first aid management of these conditions.
The common causes of acute red eye are conjunctivitis and trachoma, corneal ulcer, acute iritis, acute glaucoma and injury (or trauma). Red eye may also be due to the use of harmful traditional medicines for other eye conditions. This article deals mainly with first aid (primary level) management of red eye, which is not due to an injury.
Conjunctivitis
Conjunctivitis affecting all ages
This is the most common cause of red eye.
It is usually painless and characterised by pussy or watery discharge. There are different types of conjunctivitis: bacterial conjunctivitis caused by a bacterium e.g. Staphylococcus or Streptococcus; viral conjunctivitis caused by a virus e.g. herpes simplex; and allergic conjunctivitis caused by allergy e.g. smoke, cosmetics, medicines, etc. The signs vary depending on the cause but include swollen eyelids, red conjunctiva and a watery or pussy discharge. The cornea and pupil are usually normal.
Management
Conjunctivitis normally does not affect vision and is simple to treat. To treat bacterial conjunctivitis, clean the eyes and apply any topical antibiotic. In the absence of any antibiotics, merely cleaning the eyes of discharge regularly will allow the eyes to settle in a few days.
Usually no treatment is required for viral conjunctivitis but an antibiotic ointment can reassure the patient. Viral conjunctivitis may occur in epidemics, affecting many people at the same time. For example, a single school child with this condition could infect half the school in just one day. In cases like this it is better to close down the school for a couple of days to avoid its spread. This condition is popularly known in West Africa as ‘Apollo’. The danger is use of harmful traditional medicines, which may make the eye worse.
Allergic conjunctivitis (sometimes called vernal conjunctivitis or vernal keratoconjunctivitis) usually has a long history of intense itching of both eyes. Chronic vernal conjunctivitis gives the child’s eyes a dark brown appearance. In very severe cases these children will need topical steroids prescribed by a specialist. Steroid eye preparations can be dangerous and should only be prescribed by an eye specialist.

Conjunctivitis of the newborn
Any eye infection in the first 28 days of life is known as neonatal conjunctivitis or ophthalmia neonatorum. If this is due to Gonococcus, it is serious. The eyelids are very swollen and pussy, the conjunctiva is red and may be blood stained, the cornea is usually clear (but a white spot on it could be an ulcer which is serious and needs urgent referral).
Management
Clean the eyes gently with clean water or normal saline and apply tetracycline ointment hourly. If the cornea is involved, refer to an eye centre where the baby will
be treated with intensive antibiotic eye drops and, sometimes, systemic antibiotics.
Prevention
All babies should have their eyes cleaned immediately after birth, and tetracycline ointment applied. During antenatal care, all mothers with vaginal infections should be treated. Educate traditional birth attendants, community health workers, and both parents as this is often a sexually transmitted disease.
Corneal ulcer
Corneal ulcers have many causes. They can be caused by infection – bacteria, fungus, virus or acanthamoeba, or malnutrition, as in measles/vitamin A deficiency, which occurs mainly in infants between the ages of six months and two years. Some causes are mainly unilateral whereas others like vitamin A deficiency are often bilateral. The result of a corneal ulcer can be a corneal scar or phthisis bulbi.
A break in the corneal surface is known as a corneal abrasion/erosion/ulcer. For simplicity we will refer to all lesions as ulcers. There are superficial and deep ulcers. The patient will complain of a red painful eye.
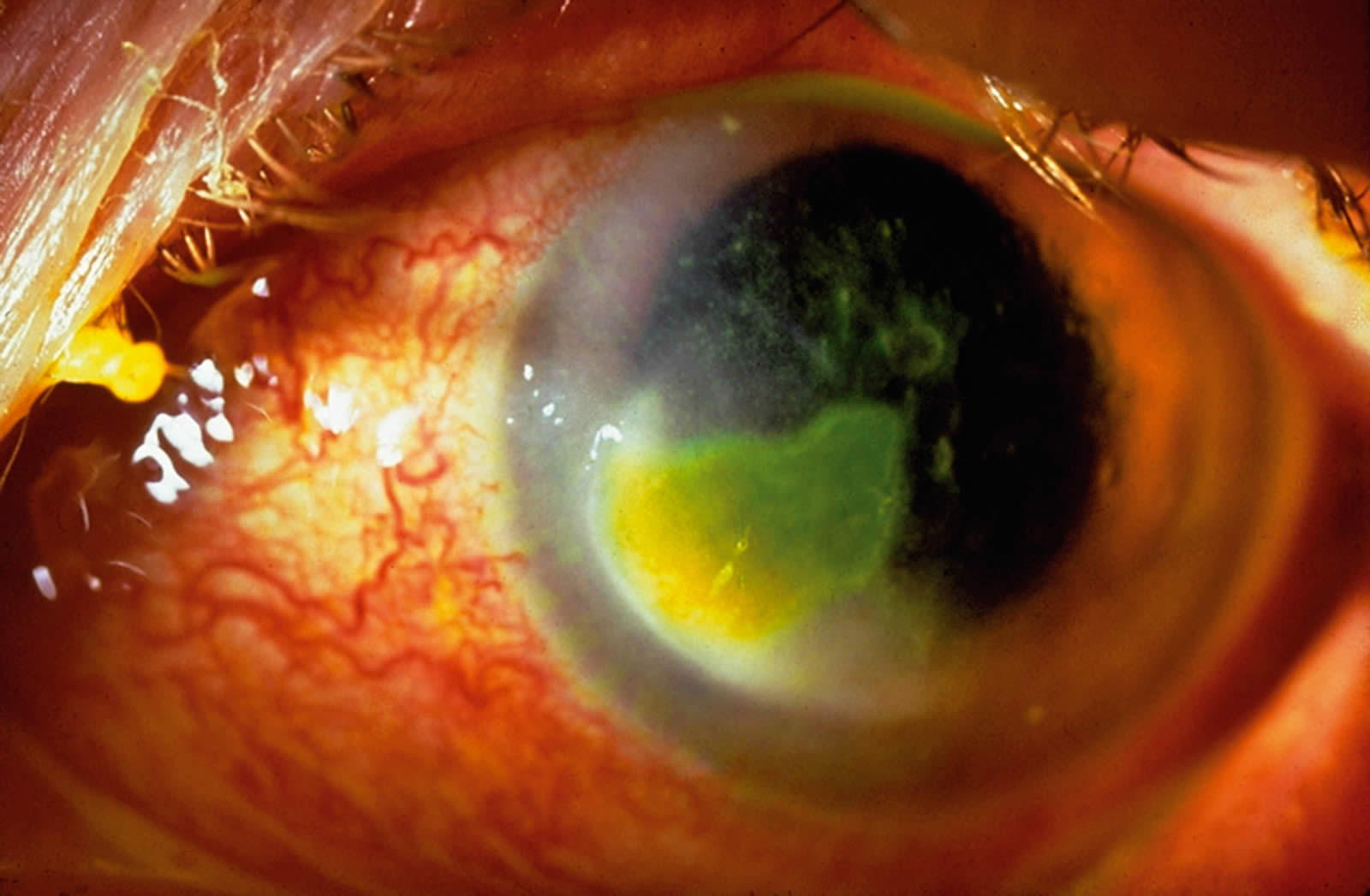
The eyelids may be swollen, the conjunctiva is red around the cornea, the pupil is normal, and the visual acuity is often reduced. There is often a grey spot or mark on the cornea. The other eye is usually normal. There is a special test to identify corneal ulcers: a fluorescein strip is placed just inside the lower eyelid and this will stain and outline any break in the epithelium a green colour. See page 79 for how to do this.
Management
Corneal ulcer is a serious eye problem. Frequent (hourly) antibiotic eye drops should be instilled, an eye pad applied, and the patient referred for help urgently. If the patient is aged one to ten years, Vitamin A 200,000 IU should also be given orally. All corneal ulcers should be managed by an eye specialist as they can easily lead to corneal scarring and blindness.
The specialist will diagnose the cause and manage appropriately. Bacterial ulcers are treated with topical and sub-conjunctival antibiotics. Fungal ulcers are treated with antifungals e.g. natamycin, but are difficult to treat. Viral ulcers are treated with anti-virals e.g. acyclovir. Nutritional ulcers are usually due to Vitamin A deficiency following measles or malnutrition. Treatment involves giving Vitamin A capsules according to age.
Acute iritis
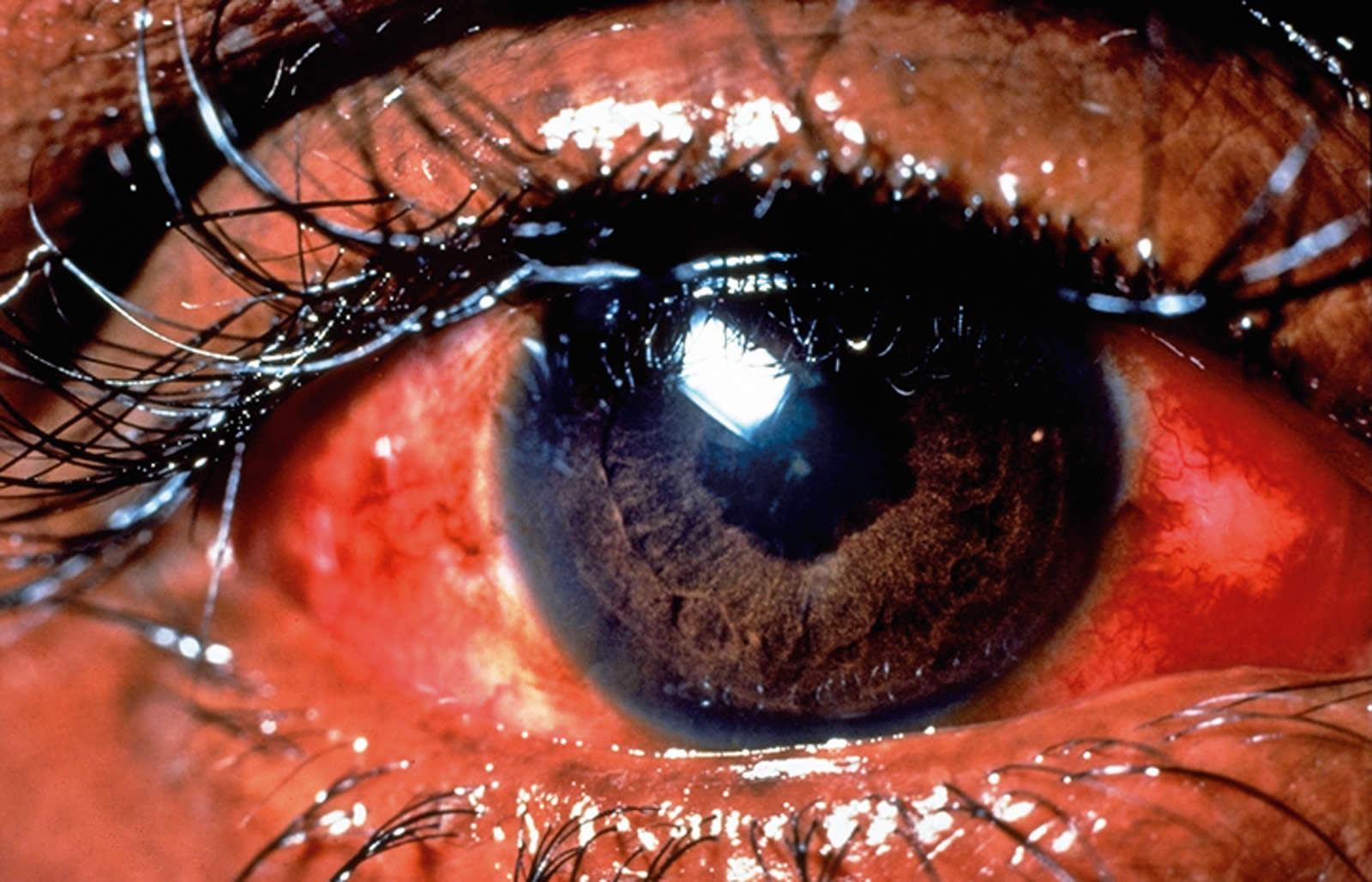
Acute iritis is often of unknown cause. The patient will complain of a red painful eye. There is no discharge but the visual acuity is reduced. The conjunctiva is red but the cornea is clear. The pupil is usually small and may be irregular in shape – this is more obvious as the pupil dilates with treatment.
Management
This is a serious problem. If you can dilate the pupil with a short-acting mydriatic, such as tropicamide, this should be done and refer the patient quickly for help.
Acute glaucoma
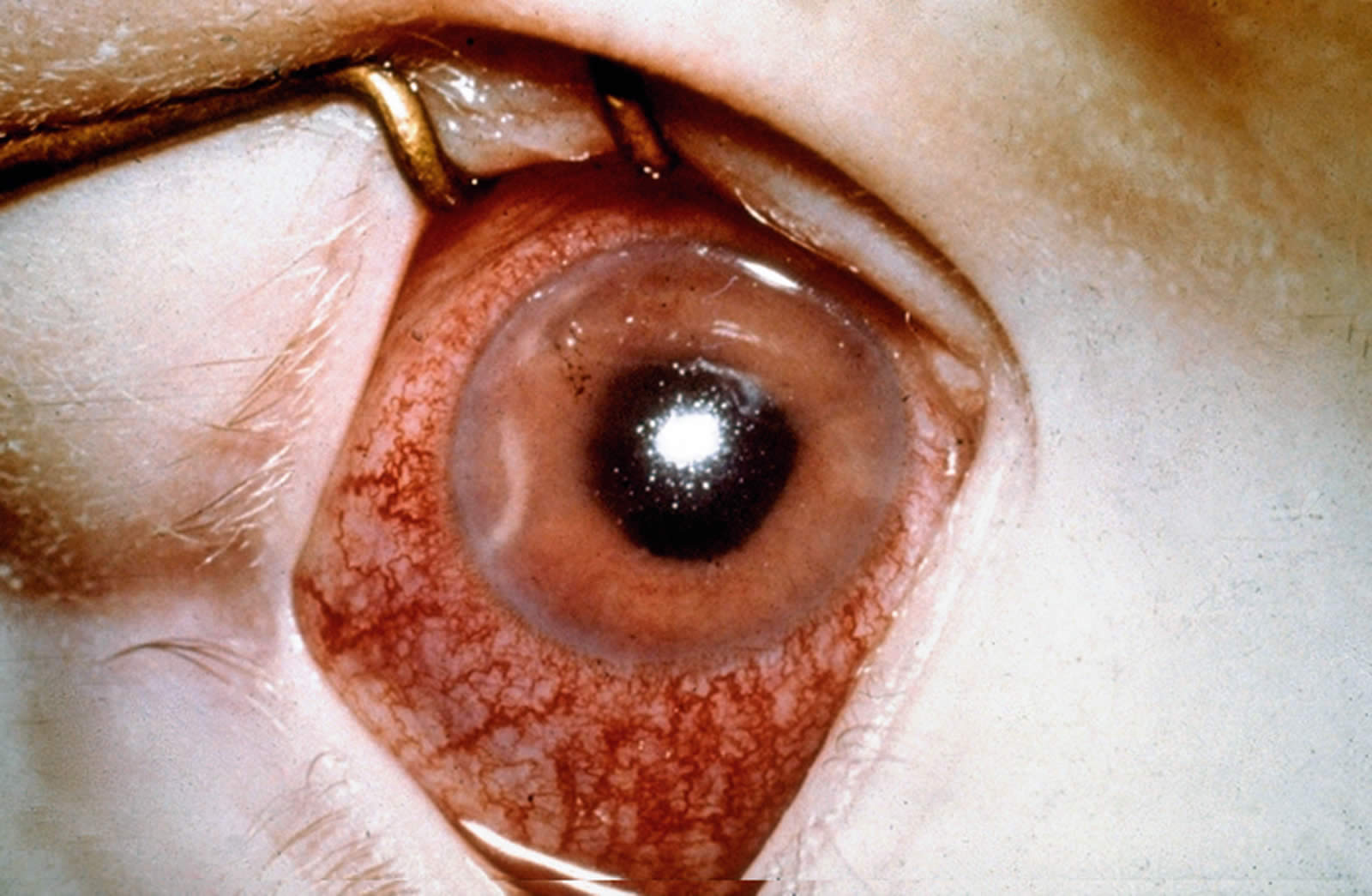
This disease is uncommon in people of African origin but more common in people from Asia. In acute glaucoma, the pressure in the eye goes up very quickly. This causes a red very painful eye, with poor visual acuity. The cornea is hazy due to oedema and the pupil is large and does not become small when a bright light is shone into the eye.
Management
This is a very serious and painful disease. The patient must be referred for help immediately. If you have diamox tablets (250 mg each), give two tablets by mouth and one tablet four times a day and refer the patient. Pilocarpine eye drops can be given (if available) to make the pupil small.
Traditional eye medicine
Traditional medicine is as old as man himself. Traditional healers are highly respected members of each community. Many patients who present at an eye clinic in Africa would have had some form of herbs or concoctions applied in his/her eyes before coming to us. This is especially dangerous in children.
Traditional eye treatments can be classified as harmful or harmless. Harmless eye treatments include incantations by traditional healers and use of salt solution, to name a few. Examples of harmful eye medicines include alcohol, ground cowries, donkey and cow dung, herbal preparations, human sputum, bird and lizard faeces, urine, etc. Eye care workers around the world would probably be able to add to this list from their own experience, and these concoctions differ from one culture to another. The preparations put into the eye can cause corneal ulcers or worsen existing ones and end up as scars or eye perforations leading to blindness.
The primary eye worker has an important role to play in preventing blindness from the use of traditional eye treatments. They are often the first point of contact when something goes wrong with the treatment, and they are also close enough to the community to discourage their use. The first step to preventing blindness from traditional eye medicines is to establish trust and respect between health care providers and patients and communities.
It is important to understand the reasons why people use traditional eye treatments, and not to judge them. There is widespread ignorance about the dangers of self-treatment for eye conditions. Many poor patients are put off seeking help from health clinics because of the negative attitudes of some health workers. Socio-cultural beliefs in evil spirits and witchcraft may lead people to think that the best course of action is with spiritual rather than medical healers; for many patients, prescribed eye medicines are considered very expensive. Furthermore, the distance to health facilities result in patients taking help from the nearest source.
Management
Most patients tend to come to hospital when the eye is already damaged. Treatment is with water irrigation, if the traditional medicine was recently applied, and then topical hourly antibiotic eye drops.
Every opportunity should be used to educate people and discourage the use of traditional eye medicine, for example, health education in communities, schools, women’s groups and clinics. Refer all patients with eye complications.
Injury (or trauma)
Traumatic injuries form about 10% of all red eyes. These injuries may cause irreversible damage to the eye leading to blindness. Many of these would need immediate referral to a secondary or tertiary eye care facility. First aid management of red eye with injury at the primary level will be covered in a future issue of the journal, and so is not included here.
Differential diagnosis of red eye with no injury
| Conjunctivitis | Corneal ulcer | Acute iritis | Acute glaucoma | |
|---|---|---|---|---|
| Eye | Usually both eyes | Usually one eye | Usually one eye | Usually one eye |
| Vision | Normal | Usually decreased | Often decreased | Marked decrease |
| Eye pain | Normal or gritty | Usually painful | Moderate pain, light sensitive | Severe pain (headache and nausea) |
| Discharge | Sticky or watery | May be sticky | Watering | Watering |
| Conjunctiva | Generalised (variable) redness | Redness most marked around the cornea | Redness most marked< around the cornea | Generalised marked redness |
| Cornea | Normal | Grey, white spot (fluorescein staining) | Usually clear, (keratitic precipitates may be visible with magnification) | Hazy (due to fluid in the cornea) |
| Anterior chamber (AC) | Normal | Usually normal(occasionally hypopyon) | Cells will be visible with magnification | Shallow or flat |
| Pupil size | Normal and round | Normal and round | Small and irregular | Dilated |
| Pupil response to light | Active | Active | Minimal reaction as already small | Minimal or no reaction |
| Intraocular pressure (IOP) | Normal (but do not attempt to measure IOP) | Normal (but do not attempt to measure IOP) | Normal | Raised |
| Useful diagnostic sign / test | Pussy discharge in both eyes | Fluorescein staining of the cornea | Irregular pupil as it dilates with drops | Raised IOP |
First aid management of a red eye with no injury
| Conjunctivitis | Corneal ulcer | Acute iritis | Acute glaucoma |
|---|---|---|---|
| Discharge in both eyes with clear cornea and normal pupil | White spot or mark on the cornea which stains with fluorescein | Small pupil which becomes irregular as it dilates | Very painful eye with poor vision and dilated pupil |
| Treat | Refer | Refer | Refer |
| Antibiotic ointment x 3/day for 5 days.
Advise on hygiene |
Hourly antibiotic drops or ointment | Dilate the pupil if possible | Oral diamox 500 mg and pilocarpine drops if possible |
Sources
Sutter E, Foster A, and Francis V. Hanyane: A village struggles for eye health, Part 2: Common eye diseases for village health workers. Part 3: Lecture notes on common eye diseases for ophthalmic assistants. London: International Centre for Eye Health. 1989.