")
Retinopathy of prematurity: clinical aspects
Related content
Retinopathy of prematurity (ROP), earlier known as retrolental fibroplasia, has become a disturbing and important cause of preventable childhood blindness.
Advances in neonatal care have led to the survival of very small babies, however, a lack of adequate ophthalmic back-up to screen all such newborn babies (neonates) for ROP has resulted in disastrous ocular morbidity and mortality.
Historical background
The belief that premature children may suffer a retinal disease, primarily as a complication of prematurity, was advanced in 1942 by Terry when he described ‘retrolental fibroplasia’ for the first time.1 The disease was probably present even before the 1940s as retinal changes consistent with ROP have been seen in the peripheral retina of people more than 75 years old, with a history of prematurity. The term ‘retinopathy of prematurity’ was first suggested by Heath in 1952.2
A national co-operative study was started in the USA in 1953 to determine the number of infants being blinded by retinopathy of prematurity. Results from 18 participating centres revealed that the incidence of ROP had a positive association with the use of oxygen for premature babies. Paediatricians were told to restrict oxygen to minimal amounts required for the survival of these infants.3 A panic reaction swept nurseries resulting in a noticeable reduction in the use of oxygen causing an increase in illness and mortality in premature babies in the 1960s.
Though the incidence of ROP fell sharply during this period, the recognition of increased paediatric morbidity and mortality swung the trend back in favour of increased use of oxygen resulting in a second epidemic of ROP from the late 1960s to the early 1980s.
In the 1980s it was seen that infants weighing less than 1000 grams, often with normal arterial oxygen levels, developed ROP and contributed to most of the cases. This led researchers to doubt the earlier concept that oxygen administration alone is responsible for ROP. They referred to studies where infants developed ROP without any oxygen administration.4 Even infants with cyanotic heart disease and very low blood levels of oxygen developed ROP, as did babies suffering from hypoxia (lack of oxygen). Thus it was realised that perhaps prematurity itself was a significant aetiological factor in causing ROP while other factors like oxygen therapy could aggravate the disease.
The primary reason for the delay in the understanding of ROP was the absence of a universally acceptable international classification. The initial classification, by Reese et al, was based on direct ophthalmoscopy.3
It was in 1977 that the indirect ophthalmoscope was used by Kingham6 who gave a comprehensive classification, efforts which resulted in the present day International Classification of ROP.
The landmark event in the history of ROP was the International Classification of ROP (ICROP), recommended by Warren Hindle and others in 1982 and put into practice in 1984.7 The ICROP Classification is based on
(a) Severity of disease: Stages 1 to 5
(b) The area of involvement: (i) Zones I, II, III (ii) Extent in clock hours.
Who develops ROP?
There are a number of risk factors for the development of ROP.
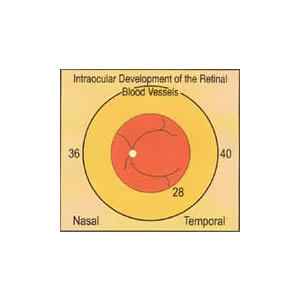
(i) Birth weight and gestational age: These are the two most important risk factors for ROP. The younger the gestational age and lesser the birth weight, the greater are the chances of developing ROP. More premature neonates are likely to develop a more severe form of disease (‘threshold disease’). – This statement has been supported by the Multicenter Trial of Cryotherapy for ROP in which 4099 infants were enrolled weighing less than 1251 gms at birth.8 This study revealed that while only 2% of babies with 1000-1250 gms birth weight developed threshold ROP, 15.5% developed this disease in the group with less than 750 gms birth weight. Similarly, while only 1.1% developed threshold ROP in premature babies of equal to or more than 32 weeks gestational age at birth, as many as 10.4% developed ROP in the group with gestational age equal to or less than 27 weeks (Diagram I).
(ii) Oxygen therapy: Though not the only aetiological agent, as it was once thought to be, excessive use is an important contributory factor. It has been seen that premature neonates develop ROP even without being exposed to oxygen and, conversely, others do not develop ROP despite being on oxygen for prolonged periods.9
(iii) Other factors: A number of other risk factors in the development of ROP include sepsis, multiple blood transfusions, multiple births, hyaline membrane disease, use of aminophylline, antibiotics, apnoeic spells, low pH, ultraviolet light therapy, etc.9
Table 1. Severity of disease
| Stage 1 | Demarcation Line | A line that is seen at the edge of vessels, dividing the vascular from the avascular retina (Fig. 1) |
|---|---|---|
| Stage 2 | Ridge | The line structure of stage 1 acquires a volume to form a ridge with height and width (Fig. 2) |
| Stage 3 | Ridge with extra-retinal fibrovascular proliferation | The ridge of stage 2 develops more volume and there is fibrovascular proliferation into the vitreous. This stage is further subdivided into mild, moderate and severe, depending on the amount of fibrovascular proliferation (Fig. 3) |
| Stage 4a | Subtotal retinal detachment not involving the macula | A self explanatory stage, occuring as a result of exudation from incompetent blood vessels or traction from the fibrous (cicatricial) tissue |
| Stage 4b | Subtotal retinal detachment involving the macula | With this stage onwards prognosis for vision becomes poor |
| Stage 5 | Total retinal detachment which is always funnel-shaped | The funnel is divided into anterior and posterior parts allowing four subdivisions, depending upon whether the funnel is open or narrow in both the parts (Fig. 4) |
Plus Disease: Another indicator of severity which reflects progressive vascular incompetence seen clinically as (a) posterior polar vascular dilatation compared with a standard fundus photograph (b) pupillary rigidity (c) vitreous haze
Screening
The lack of trained personnel for ROP screening requires us to develop clear screening criteria such that by examining a minimum number of premature neonates we are able to detect potential cases of ROP.
(i) Who should be screened?: Various centres around the world follow different screening criteria based on birth weight, gestational age and use of oxygen. On screening 2986 neonates, Brown et al found that only premature babies with a birth weight of less than 1600 gms, or those exposed to oxygen for more than 50 days, developed ROP greater than stage 3 and, therefore, their recommendation is to screen all such babies. 10This approach is now gaining popularity. We have been comfortable with our criteria of screening all babies less than 1500 gms birth weight and less than 34 weeks of gestational age, based on the study by Fielder et al.11
(ii) When should screening be done?: The natural progression of ROP must be understood to determine the time of screening. Other studies have clearly demonstrated that the natural history of retinal blood vessel development and the clinical course of ROP is related to the post-conceptional age and not to the post-natal age, though the latter is still being followed by some nurseries in their screening programmes.8,11 In the CRYO ROP study the median time of occurrence of stage 1 ROP was 34.3 weeks of post- conceptional age (PCA), while threshold disease was seen to occur at 33.6-42 weeks of PCA (median 36.9 weeks) irrespective of age at birth. 8,11 Similarly, Fielder et al found that Stage 1 ROP developed at 32.7-37.0 weeks (median 34.6 weeks) of post-menstrual age (PMA) and stage 3 developed at 35.6-39.0 weeks (median 37.1 weeks) of PMA. Thus, the events of ROP correlate with the age after conception and not the chronological age after birth (post-natal age).
These data also suggest that screening should be carried out at 33-34 weeks of PCA so as to detect ROP well before threshold disease develops.
(iii) Follow-up: Follow-up would depend on the retinal status at the time of each examination. The retinal blood vessels are considered to be ‘immature’ until vessels, reach within one disc diameter of the ora serrata. These vessels are further described as immature I, II or III depending upon whether they have reached zone I, II or III respectively. Weekly follow-up is adequate for eyes with immature I and II vessels without ROP, or in eyes with ROP stage 1 or 2 in zone II or zone III. A closer follow-up of every 3 days is required for all eyes with stage 3 ROP in zones I/II so as to begin timely treatment in case of progression of disease. Eyes with immature III vessels can be followed up fortnightly. Ideally all cases should be followed up till the vessels are considered ‘mature’, i.e., they have reached within one disc diameter of the ora serrata.
(iv) How should examination take place?: The initial screening for ROP should be done in the environment of the nursery. The pupils should be fully dilated with tropicamide/cyclopentolate and phenylephrine. In the CRYO ROP study cyclopentolate 0.2% and phenylephrine 1.0% were used, one drop each, twice, at an interval of 5 minutes.12 Examination was carried out 30 minutes later. As cyclopentolate is known to cause ileus or vomiting, dilatation was started 30 minutes to 2 hours before the feeding time of the neonates, to reduce the risk of inhalation of any food (or vomit). In our nursery we routinely use tropicamide 1% and phenylephrine 2.5%, one drop each, twice at 5 minutes interval, with good results. It is important to be aware that excessive use of phenylephrine could lead to hypertensive encephalopathy.
An indirect ophthalmoscope, a paediatric lid speculum and scleral indentor are essential for a thorough examination of the peripheral retina. The neonate is wrapped in a towel so that a single assistant can hold the head steady for examination. Topical anaesthesia is usually not necessary for speculum examination.
Table 2. Area of involvement: zones
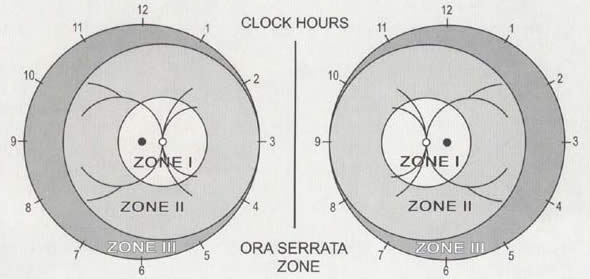
The retina is divided into 3 zones. The centre of the retinal map for ROP is the optic disc (optic nerve head) not the macula as in other retinal charts (see Diagram 2).
| Zone I | A circle is drawn on the posterior pole, with the optic disc as the centre and twice the disc-macula distance as the radius, constitutes zone I. Any ROP in this zone is usually very severe because of a large peripheral area of avascular retina |
|---|---|
| Zone II | A circle is drawn with the optic disc as the centre and disc to nasal ora serrata as the radius. The area between zone I and this boundary constitutes zone II |
| Zone III | The temporal arc of retina left beyond the radius of zone II is zone III |
| Extent | The extent is denoted by the clock hours of retinal involvement in the particular zone (see Diagram 2) |
| Rush Disease | This is rapidly progressive ROP in zone I, usually seen in extremely sick babies |
Diagram 2. Zones I, II, III and clock hours
Treatment options
When and how to treat: The CRYO ROP recommendation for the management of ROP is to treat threshold disease, i.e., the presence of stage 3+ ROP in at least 5 contiguous or 8 cumulative clock hours in zone I or II.7 The CRYO ROP study indicated poor results in 25.7% of eyes that received cryotherapy, as against 47.7% of the control eyes (P<0.0001).12 Seeing poor outcomes in about a quarter of the cases treated at this stage we, like many others, prefer to treat our cases earlier than that of the CRYO ROP study recommendation. We have had 100% good outcomes by giving treatment in patients with stage 3+ ROP in 3 contiguous or 5 cumulative clock hours in zones I or II, thus justifying our ‘over treatment’.
The aim of therapy is to treat the entire 360° of the avascular retina anterior to the ridge, either by cryotherapy or laser treatment.
Cryotherapy: The treatment should be carried out in the nursery under carefully controlled conditions. Topical or general anaesthesia may be used, the latter being preferred for the less experienced or when treating systemically unstable neonates. The entire avascular retina anterior to the ridge is given cryo applications, in two rows if necessary, using special ROP probes or paediatric retinal probes. The stress induced by cryotherapy could lead to life threatening complications. These include severe bradycardia, apnoeic spells, arrhythmias, and even cardiac arrest, thus requiring the presence of a neonatologist and full ventilatory support at all such times, especially when the procedure is being carried out under topical anaesthesia. Other problems with cryotherapy include lid oedema, conjunctival oedema (chemosis), depigmentation of skin, retinal or vitreous haemorrhage, all of which usually resolve with time.
Laser: Though the effectiveness of cryotherapy in the treatment of ROP has been firmly established, lasers (diode and argon) through indirect delivery are now being used increasingly as an alternative method of treatment with good results.13
Despite the disadvantages of laser, such as high costs, including maintenance, problems of focusing in hazy media, development of cataracts in eyes with a thick tunica vasculosa lentis (with argon laser) and longer time duration of treatment,13 it has definite advantages over cryotherapy. With the laser it is easy to treat the avascular retina, especially in zone 1 ROP, however, using cryotherapy in a similar situation may require a peritomy. Lasers cause minimal reaction and pain and fewer systemic complications.
Diode laser is preferred to argon laser because it is cheaper, easy to maintain, portable and does not cause cataracts in eyes with a thick tunica vasculosia lentis. Argon laser may be preferred by some as one can administer superficial burns with minimal pain, compared to the diode laser.
Cryotherapy however continues to enjoy its place in the treatment of ROP because of its easy availability, low cost, and portability.
Surgery: This is reserved for stages 4 or 5 disease. Scleral buckling alone may be adequate in treating stage 4a and 4b disease, however, stage 5 requires vitreo-retinal surgery which involves cutting and peeling the membranes, along with lensectomy and vitrectomy. Despite best efforts, the cost-benefit ratio is very poor with successful anatomical results in only 15-22%. 14 To quote, ‘the results are very disappointing visually and anatomically. Even years after anatomical success of surgery for stage 5, the eye may develop an hyphaema, develop new fibrous tissue and become irritable’.14
Long term follow-up: The importance of educating the parents regarding long term follow-up should not be overlooked, irrespective of what stage of ROP the child has had, as these children are likely to have refractive errors, especially high myopia, glaucoma, strabismus and retinal detachments in the future. 15
The central requirements of successful management of ROP lies in screening high risk babies at 32-34 weeks of post-conceptional age and timely intervention.
The coming generation of babies, blinded with ROP, may not forgive the attitude that many ophthalmologists adopt to avoid the painstaking effort of ROP screening. The financial, social and emotional crisis of having a blind child cannot be avoided without a committed team effort, particularly by the ophthalmologist and the neonatologist from the very beginning of life.
References
1 Terry TL: Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Am J Ophthalmol 1942; 25: 203-4.
2 Heath P. Pathology of retinopathy of prematurity, RLF. Am J Ophthalmol 1951; 34: 1249-68.
3 Szewczyk TS. Retrolental fibroplasia. Etiology and prophylaxis, a preliminary report. Am J Ophthalmol 1953; 36: 1336-61.
4 Silverman WA. Suspended judgements, memories of 1953-54 oxygen trial and its aftermath. The failure of success. Controlled Trial 1991; 12: 355-8.
5 Reese AB, King MJ, Owens WC. A classification of retrolental fibroplasia. Am J Ophthalmol 1953; 36: 1333-5.
6 Kingham JD. Classification of Retinopathy of Prematurity. In Retinopathy of Prematurity, Eds McPherson L, Hittner HM, Kretzer FL et al. Decker Inc, Toronto 1986; pp 17-25.
7 An International Classification of Retinopathy of Prematurity. Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol 1984; 102: 1130-4.
8 Palmer EA. Flynn JT, Hardy RJ, et al. Incidence and early course of retinopathy of prematurity. Ophthalmology 1991; 98: 1628-40.
9 Maheshwari R, Kumar H, Paul VK, Singh M, Deorari AK, Tewari HK. Incidence and risk factors of retinopathy of prematurity in a tertiary care new-born unit in New Delhi. The National Medical Journal of India: 1996; 9(5): 211-4.
10 Brown DR, Biglan AW, Stretavsky MAM. Screening criteria for the detection of retinopathy of prematurity in patients in a neonatal intensive care unit. J Paed Ophthalmol and Strabismus 1987; 24 (5): 212-4.
11 Fielder AR, Shaw DE, et al. Natural history of retinopathy of prematurity: a prospective study. Eye 1992; 6: 233-42.
12 Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: Three-month outcome. Arch Ophthalmol 1990; 108: 195-204.
13 McNamara J, Tasman WS, Brown GC, Vander JF. Laser photocoagulation for threshold retinopathy of prematurity. In Proc. International Conference on Retinopathy of Prematurity, Chicago IL USA 1993. Eds Shapiro MJ, Biglan AW, Miller MT. Kugler Publications, Amsterdam. 1995; pp 103-7.
14 Charles SC. Surgical results for vitrectomy for stage 5 ROP. In Proc. International Conference on Retinopathy of Prematurity, Chicago IL USA 1993. Eds Shapiro MJ, Biglan AW, Miller MT. Kugler Publications, Amsterdam 1995; pp 181-2.
15 Patz A, Palmer EA. Retinopathy of prematurity. Retina. Ed Ryan ST Vol 2. The CV Mosby Co. St Louis, 1989; pp 509-30.